

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Dextrocardia with situs inversus is rare, in which the major visceral organs are reversed, that may then lead to some confusion, as signs and symptoms will be on the 'wrong' side. Furthermore diagnosis of acute myocardial infarction and the extent of myocardial ischemia can easily be missed or underestimated unless a reversed right-sided ECG with reversed limb leads is obtained.1 There is no previous report of primary percutaneous coronary intervention (PCI) in a patient with dextrocardia and hypertrophic cardiomyopathy. We present a case of primary PCI for acute myocardial infarction in a patient with dextrocardia combined hypertrophic cardiomyopathy.
CASE REPORT
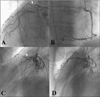
A 69-year-old male developed sudden right chest pain radiating to the right shoulder which had worsened in severity over the preceding three hours. He was a current-smoker of 60-pack-years. There was no known family history of heart disease. He visited a neighborhood hospital, where his electrocardiogram (ECG) demonstrated inverted P waves in leads I and aVL with upright P and R waves in aVR, and ST elevation in leads V1 to V3 with poor progression of R waves in the precordial leads, findings consistent with dextrocardia (Fig. 1). When he was transferred to our hospital, he was hemodynamically stable with blood pressure of 120/80 mmHg and pulse rate of 68 beats per min. Physical examination revealed a right sided apex beat. The ECG findings were consistent with dextrocardia. An ECG after limb and chest lead reversal showed ST segment elevation in leads V1 to V3 with T wave inversion in leads V4 to V6, compatible with anterior wall ST elevation myocardial infarction (MI) (Fig. 2). His chest radiography revealed right-sided cardiac silhouette and stomach gas (Fig. 3A) His two-dimensional (2D) echocardiography revealed anterior wall hypokinesia and thickened ventricular septum (16 mm) and it had abnormal myocardial texture (Fig. 3B) suggesting hypertrophic cardiomyopathy (HCMP). Left ventricular ejection fraction was preserved (55%). Laboratory tests revealed elevated levels of cardiac biomarkers: creatine kinase-MB 31.4 U/L and troponin-I 1.99 ng/mL. Emergent coronary angiography was performed after administration of aspirin and clopidogrel. Cardiac catheterization was performed via the right femoral artery with Judkins left (JL 4.0) and right (JR 4.0) diagnostic catheters (Merit Medical, Utah, USA). Baseline coronary angiogram revealed thrombotic total occlusion of the proximal left anterior descending coronary artery. There were no significant stenosis in right coronary artery and left circumflex artery (Fig. 4A, 4B, 4C). Balloon angioplasty was performed for left anterior descending coronary artery using a 2.5 mm balloon, followed by stenting using 3.5×38 mm zotarolimuseluting Stent (Endeavor Resolute® Stent, Medtronic, Minnesota, USA) at 11 atm. A repeat coronary angiogram showed stent underexpension, for which adjunctive ballooning was done using a 3.5 mm balloon at 18 atm. The final angiogram showed Thrombolysis In Myocardial Infarction (TIMI) III antegrade flow without residual stenosis (Fig. 4D). His abdominal ultrasonogram showed left-sided liver and gall bladder with right-sided spleen suggesting situs inversus totalis. He was discharged on 5th day without complication and has been followed up at the outpatient clinic.
DISCUSSION
Dextrocardia is referred to as the deviation of the heart to the right hemithorax with the axis directed to the right and caudally. There are several classifications of the condition with classification according to the viscero-atrial situs (the position of the viscera, atria and great vessels) the simplest and the most commonly adopted one.2 According to this, three types of the condition are recognized: dextrocardia with situs solitus, dextrocardia with situs inversus (mirror image dextrocardia) and dextrocardia with situs ambiguous or indeterminate.2 Dextrocardia with situs inversus occurs rarely, with an estimated incidence of 1:10000 and the incidence of congenital heart disease is relatively low, estimated to be approximately 3%.2-5 The case was also diagnosed as hypertrophic cardiomyopathy by 2D echocardiography assessment interestingly. In Korea, several cases were reported percutaneous coronary intervention in patient with dextrocardia6-9 and in one case, coronary angiogram was performed by left transradial approach.10 Although there are not a few reports of AMI in patients with dextrocardia in worldwide, there is no previous reported case of combined HCMP, to the best of our knowledge.
In patients of dextrocardia, the left-sided 12 lead ECG typically shows progressive loss of the height of the R wave from right towards the left located leads with or without loss of voltage.1 The P wave axis is a reliable indicator of viscero-atrial situs which is negative P wave axis in the left sided leads (leads I and aVL) in patients with situs inversus but positive deflection in normal individuals. These findings might be very seldom present in normal patient. On a patient with dextrocardia, ECG leads should be placed in reversed positions because reversed leads correct the negative P-wave axis and R-waves into the positive normal waves. Coronary angiography in patients with dextrocardia can be a challenge due to the abnormal anatomical location of the heart, coronary arteries and the aorta. These challenges include choice of catheters, engagement technique, radiological orientation of anatomy and appropriate radiological angles and views. The mirror image would be a good option for coronary angiography in patients with dextrocardia. In mirror-image positions, catheters can be passed using the standard technique, except that the catheters are rotated in the opposite direction for patients with dextrocardia when compared to patients with normal cardiac anatomy.
The present case emphasizes the importance of performing a reversed electrocardiogram and watchful attention in diagnosis and treatment of acute myocardial infarction in a patient with dextrocardia.



 XML Download
XML Download