

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Canine rabies continues to be a major threat in many countries especially in Asia and in Africa [1]. The disease is endemic in all provinces of Morocco except the southern desert region, with the domestic dog being the main reservoir and vector [2345] of the virus. Since 1986, about 22 human deaths have been reported yearly [6] and since 2000, an average of 376 animal cases have been recorded annually, mainly in dogs and in livestock, especially cattle [7]. The major element of rabies control strategies is regular application of injectable vaccine to reach and maintain sufficient vaccination coverage in the field enough to stop rabies virus transmission. Moroccan authorities have set up several rabies eradication plans since 1986, but to date rabies remains a serious health problem in Morocco [8]. Mass dog parenteral vaccination is an integral component of the rabies control measures [9], using an inactivated adjuvanted cell culture veterinary rabies vaccine produced locally since 1986 [2].
The mass annual vaccination campaigns are conducted in suburban and rural areas and organized locally by each district, with a vaccinator team visiting each house (door to door model) or present at several central points [10]. The dog vaccination campaigns are free of charge for dog owners and cover all the country. In urban settlements, parenteral vaccination is ensured by private veterinarians only, based on the ownership responsibility.
In view of the current epidemiological situation and of the fact that prophylactic efforts did not lead to the expected results, it appeared necessary to assess the efficacy of the vaccine in laboratory controlled conditions and also in the field. The World Health Organization (WHO) [11] recommends assessing mass dog vaccination campaigns efficacy by using well-designed serological monitoring, aiming to evaluate the vaccine potency in field conditions and also the vaccination coverage of dog population in vaccinated areas. The humoral response to rabies parenteral vaccination shows a classic profile with a latent phase, an exponential phase after first vaccination and a plateau and then a decrease in the antibody titers [12]. In primary vaccinated dogs, the seroconversion occurs generally between 4 and 6 weeks [13] and it has been shown that seroconversion is an indicator of protection against rabies [12]. In the present study, we evaluated the efficacy of the locally produced vaccine to protect field dogs in experimental conditions against a field dog rabies virus challenge. The immunogenicity of the vaccine was also investigated to evaluate vaccine effectiveness in field conditions. A blood test was performed thirty days after rabies vaccination of field dogs in eight Moroccan districts and the immunological response was measured with a WHO/World Organization of Animal Health (OIE) reference antibody virus neutralization test [14] to check seroconversion rates.
Materials and Methods
Ethics statement
All animal experiments were carried out after approval of the Moroccan national veterinary and animal welfare authority (i.e., ONSSA: 040315-15 and 110118-02) and executed by competent trained veterinarians supervised by ONSSA. All efforts were made to minimize animal suffering and strict euthanasia criteria were utilized. In all of the studied sites and regions, informed consent was obtained prior to each blood sampling from the owners, who were fully informed of the purpose of the study. Vaccination and blood sampling were only carried out with the owner or with a responsible adult representing the owner.
Vaccine
The Rabivac vaccine (Biopharma Laboratory, Rabat, Morocco) is a monovalent inactivated rabies vaccine for cats and dogs. The vaccine is produced with Pasteur virus strain on BHK21 cell culture and inactivated by beta-propiolactone then adjuvanted with aluminium hydroxide. The potency of the vaccine was checked by using the European Pharmacopeia test [15] and the antigenic activity found was at least two International Unit (IU) per dose. The vaccine was conditioned in glass vials of 5 mL (5 doses) and stored between 2℃ and 8℃ until use. The manufacturer recommended a primo-vaccination of two shots of 1 mL each within 30 days on healthy animals and a yearly booster shot.
Dogs
First experiment
Thirteen stray dogs (7 males and 6 females), aged between 3 and 6 months, and issued from the local common breed were collected in Rabat city with the collaboration of Rabat municipality veterinary service. They were housed collectively until the challenge where they were placed individually. A quarantine and acclimatization period of 9 months was observed prior to the start of the experiment. Every dog was implanted subcutaneously with a micro-chip on the left shoulder for individual identification. Dogs were fed an industrial dog food ration once a day and provided with water ad libitum. Dogs did not receive any treatment before vaccination.
All dogs were assigned to two groups randomly: group V dogs (5 males and 3 females) were vaccinated whereas group C dogs (2 males and 3 females) were the non-vaccinated controls. Two serum samples were taken from all dogs at reception in the experimental station and before vaccination and tested for rabies antibodies. Dogs were bled at the jugular vein. Sera were stored at -20℃ until analysis.
Second experiment
A total of 919 owned dogs randomly chosen older than 3 months of age living in eight Moroccan districts (Fig. 1) Agadir-Chtouka (CHT), Beni-Mellal (BEN), Casablanca (CAS), Khemisset (KHEM), Oujda (OUJ), Settat (SET), Sidi Kacem (SIDIK), Skhirat-Temara (SKT) were identified with a collar in collaboration with local veterinary services and local population. They were not pretreated for internal parasites.
Vaccine administration and blood sampling
First experiment
Dogs of group V were vaccinated subcutaneously with 1 mL of Rabivac at day 0 (D0) and at day 30 (D30). Dogs from group C were not vaccinated and were kept as controls.
Dogs of both groups were bled at D0 and at days D7, D14, D21, D28, D35, D49, D56, D64, D70, D77, D84, D91, D98, D105, D112, and D119 post-vaccination.
All sera were stored at -20℃ until the analysis of rabies antibodies.
Challenge phase and clinical observation
A challenge was undertaken on first experiment dogs 4 months (D121) after the primo-vaccination as requested by the international organizations to evaluate the efficacy of the vaccine in the target species [1516]. The challenge virus was a canine rabies strain homogenate named 'Ariana' obtained in Tunisia from salivary glands of a naturally infected dog [17]. The strain was stored in liquid nitrogen until use. The day of challenge (D121), one ampoule of virus was thawed under cold running water. A dose of 1 mL of 105.6 MIC LD50 (MIC LD50, mouse intracerebral lethal dose 50%) was injected into the left temporal muscle of each dog. The titer of the virus was verified by back-titration in mice on the day of challenge in seven groups of five Swiss mice each intracerebrally injected with 0.03 mL of different dilutions of the virus to be tested.
Dogs were clinically monitored by a veterinarian twice a day for 70 days after the challenge. Necropsy was undertaken for dead dogs and brain samples were stored at -80℃. At the end of the observation period, all surviving dogs were humanely euthanatized by using pentobarbital overdosis (Dolethal, Vetoquinol Inc., Lure, France). All brain samples were screened for the presence of rabies virus antigen by the immunofluorescence antibody test (FAT) [18] and confirmed by the mouse inoculation test (MIT) [18] in case of FAT negative result. Double smears taken from Ammon's horn, cerebellum, cerebral cortex, and medulla oblongata were stained with a fluorescent conjugate specific for rabies virus nucleocapsid (BioRad Inc., Marnes-la-Coquette, France).
Rabies virus neutralizing antibodies
The titration of rabies virus neutralizing antibodies was carried out by using the fluorescent antibody virus neutralization test as previously described [14]. The WHO Second International Standard for Rabies Immunoglobulin (NIBSC, Potters Bar, UK) was used as a positive control and the 96-well microplates were stained by using a fluorescein isothiocyanate anti-rabies monoclonal globulin conjugate (Fujirebio Diagnostic, Malven, PA, USA). The antibody titers of serum samples were expressed in International Unit per milliliter (IU/mL) by comparing results obtained with those of the positive standard included in each test. A threshold of positivity of 0.24 IU/mL has been used as done in previous studies [1419202122].
Statistical analyses
Excel 2007 Software was used to carry out calculations and graphics. R software (version 3.1.1) was used to conduct the non parametric Wilcoxon test (U test). The Bernouilli test (α=0.05) and the χ2 test were used to compare proportions obtained between different regions. All statistical analyses were undertaken with a 95% confidence limit.
Results
Kinetics of rabies virus neutralizing antibody responses of dogs maintained under experimental conditions
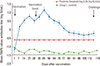
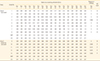
Table 1 and Fig. 2 show the kinetics of rabies virus neutralizing antibodies of individual dogs in groups V and C. Seven out of eight vaccinated dogs seroconverted as soon as 7 days post-vaccination and all dogs (8/8) developed a positive serological response 14 days after vaccination with titers higher than the threshold of 0.24 IU/mL (geometric mean, 3.34 UI/mL). Vaccinated dogs showed the maximum antibody levels 3 weeks (D21) after primo-vaccination with mean titer up to 5.81 IU/mL. Three weeks after the booster shot (D49) the maximum level of mean antibodies 13.31 IU/mL was achieved. From two months after the primo-vaccination, the humoral response became significantly weaker and decreased regularly to reach an average rabies antibody titer of 0.57 IU/mL 4 months after vaccination.
Resistance to rabies challenge of dogs maintained in experimental conditions: detection of rabies virus
The back titration of the inoculated challenge virus suspension on mice led to a titer calculation of 105,61 DL50 ICS/mL. After virus challenge of all dogs 121 days after the primo-vaccination, four out of five dogs from group C showed a variety of rabies symptoms (anorexia, curiosity, prostration, paresis, paralysis, trembling, vomit, and dyspnea). The dogs succumbed between 17 and 27 days after rabies challenge (Table 1). One surviving challenged animal (male dog No. 9) remained healthy and did not present rabies clinical symptoms.
All but one dog of group V (male dog No. 4) survived the challenge and remained healthy throughout the observation period (Table 1). The vaccinated dog that died succumbed 58 days after challenge. This dog did not exhibit any clinical sign suggestive of rabies. This dog seroconverted rapidly after vaccination and all titers measured during the kinetic study revealed the presence of rabies antibodies despite a negative titer (0.04 IU/mL) 28 days after primo-vaccination. In view of results found during all the kinetic study for this dog and of our experience with rabies antibody testing, we assume the fact that this result constituted an aberrant one, probably due to a mistake during the test. Unfortunately, volumes were insufficient to repeat the serological test.
Rabies was confirmed by FAT in all four dogs from the control group that had succumbed to the challenge. The FAT was negative in the different examined brain smears of the control dog (No. 9) that survived the challenge. The mice inoculation test failed also to detect rabies virus in brain sample and the necropsy did not reveal any particular finding.
Dogs that survived the virus challenge were euthanized and brain samples were analyzed by FAT and MIT. No virus was detected in the brain of surviving seven vaccinated dogs. The brain tissue sample from the vaccinated dog (No. 4) which died was negative by FAT for rabies antigen in the different examined brain smears. The MIT confirmed this result as it failed to detect rabies virus in the brain samples. The necropsy of the animal revealed a mesenteric torsion accident.
Serological response of owned dogs
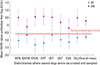
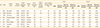
The assay conducted on owned dogs involved a total of 919 dogs vaccinated by the parenteral route in eight different Moroccan districts. The Table 2 and Fig. 3 record the distribution of vaccinated dogs within the districts and the percentages of dogs that developed positive rabies antibody response after vaccination.
At the start of the assay (D0), positive percentages of serological responses ranged from 7% in Sidi Kacem to 50% in Settat. At D30, the positive serology percentages ranged from 78% in Settat to 98% in Chtouka (Table 2). On an overall basis, 24% of dogs were positive at D0 and 92% of them were positive 30 days post-vaccination. Highest seropositive percentages (α=0.05) were found in the suburban regions at D0 (29%) and also at D30 (96%) as compared with urban areas (D0, 17%; D30, 83%) and with rural areas (at D0 [20%] only; at D30 [93%], the difference was significant with the value of the urban areas). The increase in rabies antibody titers at D30 (Fig. 3) was highly significant in all districts (p<0.001).
It should be noted that missing serological data were registered in overall population for 11.6% dogs at D0 and 16.6% dogs at D30, likely because of insufficient serum sample, hemolysis of the sample or loosed sample.
Discussion
In Morocco, many efforts are deployed in infected areas to fight against the disease based essentially on mass canine vaccination campaigns and dog population control [3]. The parenteral dog vaccination using injectable vaccines is the gold standard tool recommended by OIE [15] and WHO for effective rabies control in dogs [1011]. A vaccination coverage of 70% of the dog population is considered to be a critical threshold to achieve this goal [1123]. The rabies vaccine to be used should be approved by the national regulatory authorities according to relevant high quality international standards [111516].
Rabivac is a locally produced inactivated rabies vaccine in use in mass dog vaccination campaigns in Morocco. In this study, its efficacy was assessed in experimental conditions comparable to those of the European Pharmacopeia monograph [16], which requires a virulent challenge of the target species following vaccination. In addition, a field experiment organized in eight Moroccan districts was undertaken to check the immunogenicity of the vaccine in owned dogs.
All dogs maintained under experimental conditions were collected in the field at early age (between 3 and 6 months old), housed in an experimental kennel and kept for a long quarantine period (9 months) prior to be vaccinated since their health status as regards rabies was unknown. All dogs had negative rabies serology (<0.24 IU/mL) at D0 except dogs Nos. 4 and 11 that had a titer ≤1.15 IU/mL. The serum samples were pre-diluted prior to serological testing because of insufficient volume, hence the exact value of the titer was impossible to calculate and the immunological status (positive or negative) was therefore unknown. All vaccinated dogs seroconverted with titers above 0.24 IU/mL as early as 14 days post-vaccination (geometric mean, 3.34 IU/mL). This is similar to the findings of other authors [2425] who tested another commercial vaccine produced with the same virus strain and who found a mean antibody value of 2.53 IU/mL [26] and 5.0 IU/mL [24] 2 weeks post-vaccination in laboratory dogs. The same finding was demonstrated 1 month after vaccination, just before the boost, with a mean antibody levels of 3.10 UI/mL in our study compared with 2.03 UI/mL in the study of Minke et al. [26] and 2.8 IU/mL in the study of Kallel et al. [24] on laboratory dogs. Two weeks after the boost vaccination (D49), all dogs had high serology titers with a maximum of 41.59 IU/mL indicating an adequate immunization. The mean serological titer of the vaccinated dogs 4 months after vaccination (D119) was 0.57 IU/mL, with a high number of dogs still positive (5/8) for rabies antibody detection, contrary to previous studies demonstrating a decrease in time in rabies antibody levels in laboratory and owned field dogs primary vaccinated with one dose of commercial vaccines [242526272829]. The longer persistence of detectable rabies antibodies in this study is due to the boost one month after vaccination. After the rabies virus inoculation, one dog (No. 4) died without any symptoms or necropsy findings related to rabies. The kinetics of the rabies antibody response of this dog was similar to that of other dogs. Rabies diagnosis using FAT and MIT provided negative results. The death was not due to rabies but to a torsion mesenteric accident observed during the necropsy of the animal. All other vaccinated dogs survived, demonstrating the ability of the vaccine to protect dogs against a challenge virus of dog origin, as it would happen in field conditions.
All dogs of group C had negative serology during all the experiment except dog No. 11 who had a titer ≤1.15 IU/mL at D0. The serum was pre-diluted prior to serological testing as its volume was insufficient, as for the serum D0 of dog No. 4 (see above). Therefore, the status (positive or negative) could not be determined. All other antibody titers of this dog during the experiment were clearly below 0.24 IU/mL. This dog died of rabies 17 days after the challenge, i.e., in the same time range than other control dogs, suggesting this dog was presumably not vaccinated. A percentage of 80% (4/5) of control dogs died from rabies between 17 and 27 days after challenge, which corresponded to the classic rabies incubation period generally reported in experimentally infected dogs [173031]. The observed symptoms were in concordance with rabies clinical signs described by the OIE [15]. The 80% mortality rate observed in the control group is in conformity with the requirements of WHO, OIE, and European Pharmacopeia [111516] for validating the assay. The results of other studies using the same rabies vaccine strain [25] showed a comparable level of protection after a rabies virus challenge of vaccinated dogs. Our results demonstrate the ability of the tested vaccine to induce a high specific humoral response and full protection of field dogs against a dog rabies virus challenge.
Of 919 serologically field owned dogs sampled in urban, suburban, and rural areas, an overall of 24% harbored a positive serological response before vaccination, likely as a result of residual antibody level of a previous vaccination. Unfortunately, the dates of the last vaccinations before D0 were unknown. At D0, depending on districts, seropositive percentages varied with the highest levels obtained at Settat, Khemisset, and Oujda (50%, 48%, and 28%, respectively) and the lowest levels found at Sidi Kacem, Casablanca, and Choutka (7%, 14%, and 16%, respectively). The vaccination coverage in rural (20%) and suburban areas (17%) were statistically similar while it was statistically higher in suburban areas (29%); however, these results suggest globally that no significant difference seems occurring between the geographical status of the regions on the seropositive results obtained. The Sidi Kacem province seemed to be less covered by mass parenteral vaccination campaigns at the date of the experiment. It should be noted that the cumulative numbers of human and animal rabies cases in this province are among the highest within the country [37]. The seroprevalence percentages determined before vaccination provide a picture at a certain time of the level of detectable residual antibodies in dogs sampled in the different areas. The time elapsed between the last vaccination of each dog and the blood sampling at D0 was unknown. The curve of rabies antibodies after primary vaccination of laboratory or field dogs has been largely described (for review, see [12]) and consists in a rapid production of specific antibodies after the first vaccination followed by a regular decrease then a new rise after a booster to obtain a higher level then a new decrease but with a higher level than that previously achieved. The peak of rabies antibodies is generally observed between 3 and 6 weeks post-vaccination [121326]. A detailed review analysis of the significance of seroconversion results coupled to those of the probability of surviving a challenge has clearly demonstrated that animals seroconverting at a certain time after vaccination have a very high probability of surviving in case of rabies infection, even if they have no more detectable antibodies at the time or before the challenge [12]. Therefore, the interpretation of seroprevalence results in a field dog population sampled at different times after vaccination has a number of limitations. The percentage of 24% of seropositive dogs at D0 obtained in our study is an indicator suggesting that dogs have been previously vaccinated, and probably higher vaccination coverage of dog populations existed as these dogs had seroconverted before the D0 sampling. This value corresponds to those which have been published in similar countries [53233].
At D30 post-vaccination, an overall percentage of 92% of dogs were tested positive for rabies antibodies demonstrating the vaccine was highly effective in field conditions. The vaccination coverage was estimated at the best period, i.e., 30 days after the vaccination of dogs older than 3 months of age, and results showed in all regions significant increases in rabies antibody levels before and after vaccination. In Casablanca, where 22% of dogs were seronegative at D30, of which 9% had rabies antibodies levels less than 0.1 IU/mL, demonstrating a total absence of antibody response, and the weakest levels of rabies antibodies among different regions tested were observed (geometrical mean titer, 1.21 IU/mL). The reasons for that cannot be attributed to the vaccine since a better efficacy was achieved in other regions but could be linked to human deficiencies during the vaccination and sampling steps at the date of the experiment. The negative results could also be due to unhealthy living conditions as dogs were not dewormed and maybe did not receive sufficient food. It is known that alimentation and parasitism may influence the production of antibodies [12]. Another explanation could be that the immune response of certain dogs did not already reach the 0.24 IU/mL threshold 30 days after vaccination.
The serological monitoring of dogs following the parenteral mass vaccination campaigns is no longer recommended by WHO on a routine basis [11] because of the kinetics of rabies antibodies showing a rapid decrease particularly in primary vaccinated dogs, which represent >30% of the population because of the high turnover of the dog population [533]. Field well–designed seroprevalence studies are now recommended, as done here, for assessing the efficacy of a novel vaccine or if some failures are suspected during the campaigns, such as vaccine potency or cold chain maintenance [11], at the best period after vaccination to check seroconversion dates.
In view of these results obtained on field dogs and on the literature available on this topic, it is hypothesized that a booster with Rabivac undertaken 1 month after the primary vaccination is probably not justified. A single vaccine injection carried out each year on all dogs, including puppies, as currently done in other places with available comparable commercial vaccines, should be sufficient to ensure adequate immunization of dogs. Studies aiming at estimating the dog population should be organized also in Morocco to update the knowledge of the dynamics of the population, estimated in the 1990s at 1.6 to 2 million [5].
These results demonstrated that Rabivac induced a complete protection in experimental dogs after a virulent dog rabies virus challenge and a satisfactory humoral response in field dogs living in different conditions. This vaccine is therefore adequate for mass dog vaccination campaigns against rabies in Morocco.

 XML Download
XML Download