

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
The current most fastest and common causes of fatality worldwide are the infectious diseases of which human hand-foot-mouth disease (HFMD) is among the most pandemic viral infections. It spreads through the exposure to human enterovirus-71 (HEV-71) the primary causative agent in addition to coxsackievirus. It attacked millions of children at school age between 5-10 years old since its discovery in 1969. Therefore, infection control needs novel and effective vaccines development to be approached as important tool in pre-exposure prevention and virus eradication [1,2].
The causative agent belongs to Picornaveridea, the virions are naked in 30-31 mm diameter [3]. The virus RNA has three main genotypes and many subtypes. It's continual spread in Asian Pacific region in repeated outbreaks with changes of the causative viral subtypes among the region [4]. The faecal-oral is main route of transmission through contaminated food, its incubation period about 10 days, the main signs of infection include, fever for 3-4 days followed by skin sore on hand palm, foot, mouth, and tongue [5]. Patient continues shed the virus for weeks after recovery, therefore children at school or crowded area are under high risk of getting the infection from those who looks healthy.
The highest HFMD case number in the Asia-Pacific region nowadays occurs in China, Taiwan, Malaysia, and other countries [6]. Since its discovery, it was neglected, but nowadays the virus became as the new pandemic disease after the hard effort done in polio eradication. In addition, unfortunately, commercial applicable vaccines or effective antiviral therapy is unavailable. According to World Health Organization (WHO) report (2008), the earliest HEV-71 outbreak in the Asia-Pacific region occurred in Sarawak, Malaysia in 1997, 2000, and 2006; in Taiwan and China (1998); Australia (1999); and in Singapore (2000) [7]. Enterovirus 71 (EV71) was responsible for HFMD spread worldwide and most commonly in Europe and Asia, where its outbreaks repeated occurred in Australia, Hong Kong, Taiwan, Japan, and Malaysia [8]. In the recently outbreak in Singapore, there were 18,989 cases and it's also responsible for 1.3 million cases in China as reported by the WHO (2010) [8].
The virus structure, protective proteins and genotypes
The in vitro viral permissive cell lines used in viral isolation and propagation are the same with those used for polioviruses it includes Vero or RD cells from patient stool, rectal swab, nasopharyngeal, or skin red spots with blister [9]. The virus genome consists of a single stranded positively charged RNA genome of 7.5 kB, in a single open reading frame which translates into a longer polypeptide cleaved by viral protease enzyme into three subregions named (P1, P2, P3). P1 genes encode for the structural viral capsid proteins, VP1, VP2, VP3, and VP4, while P2 and P3 genes encode for viral nonstructural proteins mainly enzymes [10]. HEV-71 virion contains surface capsid proteins that play an important role in developing postexposure viral protective immune response. Viral VP1 is considered as the most protective antigen in addition to VP2 and VP3, while VP4 positioned in the capsid interior backbone [1,11].
Since its discovery the virus has demonstrated the genetic evolution that led to emerge of large number of viral clades inform of subgenotypes named B (1-5) and C (1-5) and they distributes differently among Asia-Pacific countries [12,13]. The common subtypes in Asia-Pacific region include B5 and C4 in Taiwan; C5 in China; C1, C4, and C5 in Vietnam; and B3, B4, B5, and C1 in Malaysia [14]. Currently, HEV-71 incidence is increasing worldwide and expected to threaten as new enterovirus attack until the effective broad protective vaccine developed [15,16].
Types of EV71 vaccine types
Effective vaccine and antiviral agent are the crucial priority tools of prevention and they are on urgent demands for controlling HEV-71 epidemics. There are various types of HEV-71 vaccine trials under development applies different vaccine design and delivery strategies, examples includes live attenuated or inactivated vaccine, virus-like particle; virus VP1 recombinant and subunit vaccine expressed in viral or bacterial vector and DNA vaccine; currently one inactivated vaccine is under phase 3 trials in China and another one in Taiwan [17,18].
In vaccine developmental research, recently different types of nano-particles and micro-carriers for use in vaccine delivery to enhance their immune response through increased presentation of vaccine epitopes to the antigen-presenting cell in order to induce enhanced cellular and humeral immunity. Calcium phosphate (CaP) used as vaccine carrier adjuvant in tetanus toxoid for long-term immunization including many research work with promising result in promoting improved systemic immunity [19,20].
Vaccine adjuvants are substances added to the vaccine in order to scale up its postimmunization antibody levels compared to using vaccine alone. There are few numbers of approved adjuvants for use in human vaccines such as aluminum salts. Recently the issue of the adjuvant side effect is challenging and increased the demands for safe vaccine ingredients mainly the adjuvants used in H1N1 vaccine, question has been raised on its side effect and safety. CaP is one of those promising biocompatible self-antigen adjuvants that can induce improved immunity towards vaccine epitopes only (Fig. 1), and of a very low or no side effects because it's a natural main structural component of bones [21].
Moreover, using virus-like particle could provide better cross-protection, but its peptide conformation similarity a bit varies not only from the native virion particle of the same viral subgenotype but also more variability compared to other genotypes; due to differences in post-translational modifications that take place in expressing host cells (Escherichia coli or yeast), again, the peptides produced may have less neutralizing capacity towards other viral genotypes that naturally replicate in a different somatic host cells such as cells on human epithelial respiratory and digestive tracts. In addition, its production procedure and their purification downstream increases vaccine cost [22].
Vaccine delivery adjuvant formulation of choice
The level of postvaccination immunity based on combination of many key factors such as the dose numbers, volume, route of administration, the antigenic contents, and adjuvant used. The adjuvant induced immunity differ according to the difference in adjuvant, types, ratio between the adjuvant and vaccine, the route of administration, the charge and particle size of the adjuvants, the nano-particles size adjuvant allows larger surface for an increased amount of vaccine epitopes to adsorb which in turn could enhance the delivery of the vaccine and its presentation that results collectively in higher levels of protective antibodies [17,23].
The current research in developing viral vaccines generically based on switching between vaccine types which sometimes affects vaccine capacity in term of cross-protection among viral subtypes. In EV71 disease, it seems that the proper and best way to provide preinfection protection and most importantly the vaccine's ability to induce high and protective immunity through induction of neutralizing secretory IgG antibody at in order to neutralize EV71 viral entry as preventive control measures providing a protective systemic immunity. The presence of multiple subgenotypes and more than one surface capsid protein among EV71 increased the challenge of developing a broad protective vaccine, which could be only achieved through using vaccine consists of all capsid proteins VP1, VP2, and VP3 such as an inactivated whole virion. The virus-like particle vaccine, but it has two main disadvantages on cost wise and cross-protection among viral subgenotypes [24,25].
Ongoing HEV-71 vaccine research
Vaccine effectiveness depends on its capability to provide enough protection in order to avoid infection, to minimize post-infection complications, to reduce the viral shedding or block its transmission. Most of the ongoing vaccine research designed for induction of increased systemic humoral and cellular immunity, using increased dosage volume through intramuscular route to offer high viral neutralizing IgG antibodies. In general, live attenuated vaccine could induce higher levels of protection, but the reversion of virus virulence similar that of oral polio vaccine remained possible and the issue of a vaccine safety is a priority demands before providing protection.
The use of Rec-DNA-, VP1- or DNA-based vaccines, could provide better protection, but only in narrow protection towards other viral subgenotypes due to antigenic variability in capsid outer epitopes meaning a weak neutralization and low across protection compared to that of intact killed vaccines [25,26].
The nature of easy fecal oral transmission of EV71 infection, the presence of three viral immune-protective capsid outer proteins; VP1, VP2, VP3, and presence of different EV71 viral genotypes; it's very important to develop a broad protective vaccine inactivated whole EV71 vaccine in order maintains the native peptide conformational and the structure epitopes of the virion outer capsid proteins. And it's crucial that the vaccine capable to induce strong systemic immunity and to neutralize early viremia through the presence of viral specific higher titers of IgG antibodies [16].
The introduction of intradermal vaccine adsorbed to nano-adjuvant expected to be a novel effective HEV-71 vaccine product, and it might induce highest systemic protective immunity, in a smaller dose volume and less antigenic content in improved virus neutralization [18].
The development a safer inactivated HEV-71 whole vaccine adsorbed to biocompatible nano-size CaP adjuvant particles for intradermal administration, for the induction of measurable higher postvaccination viral specific protective IgG antibodies compared to intramuscular and the unadjuvant killed vaccine, as one best potential, applicable and novel preventive mean for the preventing the pre-exposure EV71 infections. Moreover, the vaccine epitopes adsorbed to nano-adjuvant will be released at a controlled rate to the blood circulation in a prolonged availability due to the increased surface area of the adsorbing nano-adjuvant particles at distal intradermal vaccine administration site will reduce the speed of phagocytic clearance of the epitopes and increased the stimulation of the immune cell.
Materials and Methods
Cell and virus
Vero, green African monkey kidney cell lines, from ATCC (CCL-81) were prepared in 80%-85% confluence for the in vitro propagation of the virus. HEV-71 subtype A was obtained from HEV-71 (BrCr strain; ATCC, VR-784).
Virus propagation and concentration
HEV-71 BrCr virus strain was prepared I Vero cell line and the theatre was measured in the plaque assay with a virus titter of 4.6×104/mL and kelp as stock seed preserved at -80℃, the virus working seed prepared to infect cell monolayers to produce large-scale virus suspension using 75-cm2 tissue culture flasks of confluent Vero cell inoculated with 1 mL of HEV-71.
The flasks of cultured cell incubated at 5% CO2, 37℃ for 1-hour virus adsorption, then 15 mL of RPMI-1640 medium with L-glutamine 1% fetal bovine serum culture medium (Sigma, St. Louis, MO, USA) added to each culture flask. A total volume of 1.2 L of virus suspension prepared. The viral suspension clarified through low-speed centrifugation (4,000 rpm/min for 15 minutes at 4℃), the cells were pooled in 50-mL sterile falcon tube and subjected to three cycles of freeze-thawing and sonicated for 10 minutes ultrasonic water bath (Hwasin Technology, Seoul, Korea). The debris of cell lysate removed by centrifugation (4,000 rpm/min for 15 minutes at 4℃), and the released virus in supernatant kept at -80℃. The viral suspension aliquot of 35 mL was concentrated at 25,000 rpm, for 5 hours at 4℃ in a high-speed centrifuge (Avanti J25, Beckman Coulter, Fullerton, CA, USA), the virus in the bottom 3-5 mL was removed and polled. The virus was further concentrated in ultracentrifuge 35,000 rpm/min, 3 hours at 4℃ (L-100, Beckman Coulter) in 11-12 mL aliquots, the viral pelted polled and aliquots of the concentrated virus preserved at -80℃.
HEV-71 virus quantification and inactivation
The quantity of HEV-71-VP1 antigenic content monitored during the processes of virus concentration using a quantitative commercial enzyme-linked immunosorbent assay (ELISA) kit from Abiotic (Abnova-KA1677, Taipei, Taiwan). The concentrated virus stock completely inactivated using beta-propiolactone at dilution 1:2,000 for 5 hours at 4℃, under continuous agitation. The killed vaccine aliquots kept at -80℃, to use to visualize the virus size and morphology under transmission electron microscope using 1.5% uranyl-acetate dye and in preparation of vaccine formulation with adjuvant for animal immunization.
Adjuvants characterization
CaP powder from Sigma prepared by dissolving 10 mg in 100 mL of deionized water to make 10% stock and the solution subjected to continuous stirring for 6 hours at room temperature, followed by sonication for three times repeated cycles of each 15 minutes; aliquots of 2 mL were kept and samples used for characterization for the chemical and physical properties. Another commercial CaP adjuvant was donated from Brenntag Biosector (Ca. 7758-87-4, Brenntag Biosector, Copenhagen, Denmark) and was used to compare with the prepared adjuvant particles size and morphology.
Adjuvant size and cytotoxicity
Adjuvants were examined for calcium content measured by an OCPC calcium quantification kit form (Reckon Diagnostic India, Vadodara, India). The samples from the two adjuvants were examined for particles morphology under scanning electron microscope (SEM; JSM 6400, JEOL, Tokyo, Japan) for particles size and morphology, samples also were examined in Zetasizer Nano-ZS (Malvern Instruments, Worcestershire, UK) to determine adjuvant particle size and total charge. Human liver cell lines (HepG2, ATCC HB-8065) were used to examine the adjuvants inhibitory adverse effect on liver cell proliferation as an indicator of how safe to use CaP as biocompatible adjuvant in human vaccine.
Vaccine formulation, dosage, and animal immunization
The prepared HEV-71 whole vius inactivated vaccine combined with each of the two adjuvants in at a ratio of 1:1 at final calcium content 1% per each vaccine dose below that recommended by WHO (1.3%) and the final vaccine antigenic contents in each dose adjusted to 0.5 µg/mL. New Zealand rabbits (ethical approval number: UPM/FPSK/PADS/BR-UUH/00487) used to study the capacity of each adjuvant formulation using both types of CaP adjuvant, compared to the vaccine without adjuvant for induction of postvaccination immunity after its administration through both intramuscular and intradermal. Each group of rabbits consist of three animals received five injections of the vaccine at time intervals of 0, 1, 3, and 5 weeks, the groups were as follows: nano-CaP/HEV-71 vaccine intradermal and intramuscular, two groups; micro-CAP/HEV-71 vaccine intradermal, one group; and vaccine-free adjuvant intradermal and intramuscular, two groups; plus unvaccinated animal as a control group; all vaccine formulations prepared on the same day of vaccination.
Samples collection
The blood samples were withdrawn from rabbit ear venous at intervals (0, 1, 3, 5, 7, and 9 weeks); the samples were allowed to clot normally at room temperature for 2 hours, then were centrifuged and serum was collected and preserved at -80℃ for determining of HEV-71 postvaccination IgG and IgM antibodies in an in-house developed using goat anti-rabbit-horseradish peroxidase (HRP) conjugate IgG (A0545, Sigma) and goat anti-rabbit IgM-alkaline phosphate (402004, AbD Serotec, Dusseldorf, Germany).
Evaluation of postvaccination systemic antibody response
Rabbit samples were examined for HEV-71 viral specific IgG and IgM antibodies using in-house developed ELISA assay. The assay used an indirect ELISA using labelled anti-rabbit IgG-HRP and anti-rabbit IgM-HRP to detect the viral specific antibody from animal serum bound to virus antigen in 96-well plates coated with 0.5 µg/mL at serum dilution 1:200 for IgM and 1 µg/mL at serum dilution 1:400 for IgG which detected by secondary rabbit labeled HRP-conjugated and TMB color developer substrate. Plates were read at 450 nm, the developed color intensity proportionate to the postvaccination viral specific antibodies in sera was compared to the unvaccinated control group. The group mean antibody was compared with Student t-test and the threshold for significance considered with p-value of <0.05. The series of obtained mean antibody levels between the vaccinated groups and control were analyzed in One-way ANOVA statistical test (Minitab ver. 16.0, Minitab, State College, PA, USA).
Results
Vaccine preparation and inactivation
Complete viral inactivation checked in Vero cells by incubation for 6-day post-infection without viral cytopathic effects was compared to the virus infected (Fig. 2B) and uninfected cell control (Fig. 2A). The HEV-71 antigenic content was measured after each virus concentration process to validate the viral content in the final vaccine dose formulations. The virus content increased in quantity through the preparation process: from direct cell supernatant (0.3 µg/mL), after high-speed centrifugation (1.5 µg/mL), and after the ultracentrifugation (4.0 µg/mL) (unpublished data).
Virus and adjuvant electron-microscopy
CaP was prepared nano-adjuvant of 73-nm (a), commercial adjuvant of micro-size particles (1.7 µm), when visualized under SEM. The virus diameter was in same expect size diameter and morphology of HEV-71 and other none-enveloped picornaviruses (31 nm) (Fig. 3).
Adjuvant particle size
Particles size of the prepared adjuvant showed mean particles distribution of 30 nm while that of commercial CaPs were of particle size of 905 nm (Fig. 4). The difference between particles size in SEM and Zetasizer Nano-ZS (Malvern Instruments) is atriute to the method applied in visualizing drying of the sample during which calcium ion naturally agglomerated as a result of the size diameter increases as the water being removed.
Adjuvant cytotoxicity
The effect of adjuvants on the in vitro proliferation of human liver cell is examined on HepG2 cell line monolayers after its exposure to gradient concentrations of each adjuvant for 72 hours, the percentage of viable cell among all of the preparations were either equal or above 50% which indicate for the absence of adverse cytotoxic effect in both adjuvant, the percentage of cell viability elevated commercial adjuvant compared to nao-adjuvant (Fig. 5).
HEV-71 viral specific antibody response
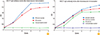
In-house ELISA was used to measure and compare the level of IgM and IgG antibodies on week 1, 3, 5, 7, and 9 postimmunization of rabbits with the HEV-71 vaccine in the following formulations and route: intradermal (nano-CaP/vaccine, micro-CaP/vaccine, vaccine without adjuvant) and intramuscular (nano-CaP/vaccine and vaccine without adjuvant and unvaccinated control group samples). The nano-adjuvant adsorbed to the vaccine elevated the IgM antibody compared to that of microsize adjuvant (Figs. 5, 6), after the third vaccine dose through both administration routes. IgM antibodies were elevated significantly in rabbits immunized with vaccine adsorbed nano-CaP adjuvant through intramuscular route, while initially micro-adjuvant showed increased level which dropped faster than the nano-adjuvant at week 5 after the third dose of vaccine (Fig. 6).
The role of adjuvant particle size on postvaccination antibody response
The nano-CaP adjuvant demonstrates its capacity of induction of highest viral specific antibody through both parenteral vaccine administrations compared the vaccine adsorbed to micro-adjuvant or immunizing with vaccine alone. The micro-adjuvant also displayed ability of inducing increased level of antibody than the vaccine alone. The IgG level was elevated in rabbits immunized intramuscular with nano-adjuvant adsorbed vaccine compared to vaccine alone.
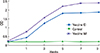
While IgG level was higher in rabbits immunized intradermal with nano-adjuvant adsorbed vaccine compared less in micro-adjuvant adsorbed and it was the least in animal received vaccine alone (Fig. 7). Systemic IgG levels between the groups of different immunization routes were higher vaccine adsorbed nano-adjuvant administered through intramuscular route (0.5 µg/mL) of 1.0-mL volume, then nano-adjuvant administered intradermal nano-adsorbed vaccine (0.5 µg/mL) and less with the intradermal micro-size adsorbed vaccine (0.5 µg/mL) of 0.1 mL volume throughout the last 6 weeks (range, 3 to 9 weeks) (Fig. 8).
While the IgG antibodies were elevated among animal group immunized intramuscular with un-adsorbed vaccine of 1-mL dose volume (0.5 µg/mL) compared to that of reduced intradermal immunized animal with 0.1-mL (one-tenth) dose (0.5 µg/mL).
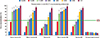
As a result, this validates and indicates for the usefulness and role of using both adjuvant adsorbed vaccine and in a nano-size particles (Fig. 9).
Postvaccination HEV-71 neutralizing systemic antibody titer in animal serum
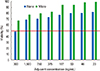
The in vitro virus neutralizing antibody titer in animal serum samples is examined in cell viability assay as an indicator for the presence of postvaccination viral specific neutralizing antibody that inhibits virus infectivity in susceptible cell line (Vero). The higher the neutralizing antibody is samples proportionate to the increased percentage of cell viability. The assay results displayed higher cell viability and neutralizing antibody in samples from the animal group immunized with intradermal vaccine adsorbed to nano-CaP adjuvant with antibody titer 1:1,600 followed by vaccine adsorbed to micro-particles CaP (1:800) compared to unadsorbed vaccine of neutralizing titer below (1:200). Moreover, among intramuscular immunized animal the vaccine attached to nano-CaP adjuvant induced elevated neutralizing antibody titer of 1:600 compared to unadsorbed vaccine animal (1:400) which considered low (Fig. 10). The neutralizing titer of the intramuscular micro-particle adsorbed vaccine was higher than that in animal received unadsorbed vaccine.
Discussion
Adsorbing HEV-71 vaccine to the CaP-adjuvant regardless to its particle size or the route of parenteral immunization has displayed a significantly elevated level of postvaccination viral specific IgG-antibody. Which makes this biocompatible adjuvant is important in the future of successfully developing preventive HEV-71 vaccines (Figs. 7, 8).
The use of nano-particles adjuvant in vaccine through intradermal immunization (0.1 mL) was able to induce highest level of viral specific antibodies compared to that of the vaccine alone through both the intradermal and intramuscular vaccine administration as an indicator for the importance of using nano-size particulate adjuvant in HEV-71 vaccination for improving the vaccine antigenic adsorption in term of quantity and the release of the epitopes to the immune cells (Figs. 7, 8, 9).
The levels of postvaccination antibody in animal group received only 0.1-mL intradermal dose of vaccine alone (0.5 µg/mL) was almost closer to the 10× intramuscular dose of 1.0-mL volume (0.5 µg/mL), indicative of the usefulness of intradermal route for vaccine administration and a potential approach for assurance of improved HEV-71 postvaccination elevated immune response using reduced vaccine dose (0.1 mL) compared to conventional intramuscular route and this could help the significant drop in vaccine dose volume (Fig. 10).
A minor elevation in IgM antibody appeared animals immunized intramuscular with nano-adjuvant adsorbed vaccine compared to the unadsorbed vaccine, while other group received intradermally does not show clear variation similar to that in IgG antibodies (Figs. 5, 6).
The nano-CaP adjuvant induced higher HEV-71 specific antibody levels compared to the vaccine adsorbed in micro-size commercial CaP, which improve and validate the crucial benefit of applying nano-size adjuvant in vaccine development generally as a novel approach. As a result, it displayed the superior advantageous of nano-size CaP adjuvant adsorbed-vaccines against HEV-71 for developing highest and protective postvaccination systemic immunity through intradermal immunization (Figs. 7, 9). Nano-CaP developed almost equal or greater antibody compared to the levels of postvaccination induced by other vaccine formulations through both of the parenteral route of immunization after 45-50 days; this indicates the role of nano-size adjuvant in adsorbing increased amount vaccine epitopes due to its increase total adjuvant surface area (Figs. 6, 7, 8, 9).
The virus neutralizing assay indicated how vaccine adsorption into adjuvant is important for the enhancement of systemic immunity in general. In addition, it has specifically indicated the role of both the smaller nano-size adjuvant and intradermal immunization in the induction of elevated and protective immunity (Fig. 10).
The intradermal route for administering HEV-71 vaccine demonstrated highly and promising immune response compared to the conventional intramuscular route, seems due to slow release of vaccine epitope and its distal locality from the circulatory and lymphatic system. It also use 0.1-mL dose volume (0.5 µg/mL) that is equal to one-tenth of the intramuscular route full vaccine dose of 1.0-mL volume, this could have a direct impact on vaccine cost increasing its affordability.
The safety of using novel nano-size CaP as the safest vaccination is compared to those commercially used adjuvants-like alum salts not only because of its biodegradability, but also due to its biocompatibility which make CaP considered self-antigen non-antigenic to the immune system. Therefore, CaP-adsorbed vaccine will only induce epitopes specific antibodies but not adjuvant specific antibody compared to incompatible adjuvants being recognized as antigens inducing specific antibodies towards both adjuvant-particles and vaccine beside the safety drawbacks of that incompatible adjuvant (Fig. 1).
In conclusion, immunization with HEV-71 vaccine through intradermal route, and the introduction of novel biocompatible safer, non-size particles, non-antigenic CaP adjuvant in HEV-71 vaccines could be the most superior promising novel strategic mean to offer a safer vaccine adjuvant and the induction of potent protection against HEV-71 in the coming decades.
The introduction of nano-based adjuvant in vaccines development could improve their effectiveness prolong the interval of boosting doses, reduces the number of doses and the antigenic content of the vaccine which collectively will have positive impact on vaccine affordability through reduction of preparative and its final market cost.
The combined use of biocompatible adjuvant could improve vaccine safety issue replacing the side effects of currently used commercial adjuvant and reducing the negative concerns about vaccines in general.
The intradermal route of immunization showed capability in offering similar levels of postvaccination antibody using only one tenth of the conventional intramuscular dose quantity and volume that will markedly reduce vaccine cost effeteness and scales up its affordability.
Future implication of the study outcomes indicate this much effective and safe nano-based CaP adjuvant could be the best choice not only for the HEV-71 vaccine, but also for developing other vaccines of an improved effectiveness and safety.






 XML Download
XML Download