

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Measles, mumps, rubella and varicella are four common and potentially serious infectious diseases in children worldwide [1-3]. Complications associated with these diseases can be serious and potentially life-threatening [1-4]. Measles and varicella are associated with serious complications leading to hospitalizations and potentially death [1,4]. Mumps commonly causes severe forms of meningitis and encephalitis [2]. Infants born to women infected with rubella in their first trimester of pregnancy are at high risk of congenital rubella syndrome, which may result in death [3,4].
In Korea, since the introduction of a combined measles-mumps-rubella (MMR) vaccine in the national immunization program, the morbidity and mortality associated with these diseases has decreased substantially [5]. Measles elimination was achieved in Korea in 2006 [6] and reported rubella cases decreased from 2001 to 2009 [7]. On the other hand, while immunization did result in a considerable decrease in mumps cases, a resurgence of mumps was observed between 2003 and 2009 [5]. Furthermore, although a varicella vaccine has been routinely administered to children (age, 12 to 15 months) since 2005, the seroprevalence of varicella continues to be relatively high (50% in children aged 1-2 years, 75% in children aged 5-6 years and 90% in individuals aged >11 years) [8].
A live-attenuated MMR vaccine, Priorix (GlaxoSmithKline, Rixensart, Belgium) and a live-attenuated varicella vaccine, Varilrix (GlaxoSmithKline) have been available since 1997 and 1994, respectively [9]. Both vaccines are recommended by the United States Center for Disease Control's (CDC) Advisory Committee on Immunization Practices (ACIP) as two doses each, with similar schedules (first dose at 12-15 months and the second dose at 4-6 years) [10,11]. These vaccines were found to be well tolerated when administered concomitantly as separate injections, and do not appear to adversely interfere with the immunogenicity of any of the vaccine antigens [12].
Considering the similar vaccination schedules for both vaccines, a combined tetravalent MMR-varicella (MMRV) vaccine that would confer protection against all four diseases was developed (Priorix-Tetra, GlaxoSmithKline). The combined MMRV vaccine is based on the licensed MMR and varicella vaccines [9] and would allow for more flexibility in incorporating the vaccine into the increasing number of scheduled childhood vaccinations [9,13-18]. Results from previous clinical studies have shown comparable immunogenicity and tolerability between the combined MMRV vaccine and concomitant administrations of the MMR and varicella vaccines [9].
In several European countries, the combined MMRV vaccine is licensed for use according to a two-dose schedule in infants aged ≥9 months, with a minimum interval of six weeks between doses [15]. In the present study, the immunogenicity and safety of a single dose of a combined MMRV vaccine in comparison to that of concomitant administrations of MMR and varicella vaccines given as separate injections was assessed in healthy Korean children during their second year of life.
Materials and Methods
Study design and subjects
This was a phase IIIb, open-labeled, randomized study (NCT00751348) conducted at 13 study centers in South Korea between October 2008 and May 2010. Healthy children aged 11-24 months, not previously immunized against measles, mumps, rubella and/or varicella and without a previous history of these diseases were randomized into two parallel treatment groups (2:1) to receive either one dose of the combined MMRV vaccine (MMRV group) or MMR and varicella vaccines concomitantly as separate injections (MMR+V group).
Subjects were excluded from participating in the study if they had received any investigational drug or vaccine 30 days before the administration of the study vaccine, if they had received immunosuppressants, immunoglobulins or any blood products six months prior to the study, if they had a history of allergy likely to be aggravated by any of the vaccine components, chronic illness or family history of immunodeficiency, or if they demonstrated symptoms of acute illness at the time of enrollment. Subjects with a rectal temperature ≥38.0℃ or an axillary temperature ≥37.5℃ at the time of vaccination could not receive the study vaccine. Finally, subjects were excluded if they resided in a household with newborn infants, pregnant women with a negative history of chickenpox or immunodeficient people.
The guidelines of Good Clinical Practice, the Declaration of Helsinki, and the local rules and regulations of South Korea were adhered to during the conduct of this study. The Independent Ethics Committee/Institutional review board of each participating center reviewed and approved all study-related documents. Parents/guardians provided written informed consent prior to performing any study-related procedures.
Study vaccines
The three study vaccines, namely, MMRV (Priorix-Tetra), MMR (Priorix), and varicella vaccine (Varilrix) were manufactured by GlaxoSmithKline, Belgium. All were supplied in monodose vials, each containing a lyophilized pellet to be reconstituted with the diluent (provided in a pre-filled syringe) as a 0.5 mL dose at the time of injection. The composition of each study vaccine is provided in Table 1. All vaccines were given subcutaneously as a single dose in the upper arm (deltoid region). Subjects were monitored for 30 minutes after vaccination in case of anaphylactic reactions.
Assessment of immunogenicity
Blood samples were collected before and 43 days (range, 42 to 56 days) post-vaccination. Antibody titers were measured using commercial enzyme-linked immunosorbent assays (ELISA)-(Enzygnost, Dade Behring, Marburg, Germany) with cut-off values of 150 mIU/mL, 231 U/mL, and 4 IU/mL for measles, mumps, and rubella, respectively. For varicella, antibody titers were measured using an immunofluorescence assay (IFA)-(Virgo, Hemagen Diagnostics, Columbia, MD, USA) with an assay cut-off value of 4 dilution-1. A post-hoc analysis was conducted for measuring anti-mumps antibody titers using the plaque reduction neutralization (PRN) assay (cut-off 24 ED50) [19].
Assessment of safety/reactogenicity
Parents/guardians used diary cards to record the occurrence of solicited local symptoms (pain, redness and swelling) at the injection site for a period of 4 days following vaccination and solicited general symptoms (fever [axillary temperature ≥37.5℃/rectal temperature ≥38.0℃], rash/exanthem, parotid/salivary gland swelling and any suspected signs of meningism, including convulsions) for a period of 43 days post-vaccination. Body temperature was measured daily via the rectal/axillary route for the first 15 days post-vaccination. Between day 15 and 42, the presence of fever was assessed using a temperature-sensitive pad (a forehead-adhering strip that measures body temperature), and if fever was suspected, an accurate measurement of temperature was performed with a thermometer. Additionally, the occurrence of unsolicited symptoms during the 43-day post-vaccination follow-up period and the occurrence of serious adverse events (SAEs) during the whole study period were recorded.
Intensity of symptoms was graded on a scale of 0-3. Solicited symptoms were defined as grade 3 as follows: 1) pain: when limb was moved or a spontaneously painful limb; 2) redness and swelling: injection site surface diameter >20 mm; 3) fever: axillary temperature >39℃ or rectal temperature >39.5℃. Unsolicited symptoms were defined as grade 3 when preventing normal daily activity.
Statistical analyses
All statistical analyses were performed using SAS version 9.2 (SAS Inc., Cary, NC, USA), and 95% confidence intervals (CI) were calculated using Proc StatXact 8.1.
Following consideration of eligible subjects, central randomization of subjects was conducted using a minimization algorithm to provide each subject with a unique treatment number. A randomized (4:2) blocking scheme ensured that the balance between treatments was maintained by providing a unique treatment number that identified the vaccine dose to be administered to the subjects. The study was conducted in an open manner considering the differences in the physical characteristics of the study vaccines and number of injections between the MMRV and MMR+V groups.
The sample size was calculated taking into consideration the primary non-inferiority objective. The primary objective of non-inferiority was met 43 days post-vaccination, if the lower limit of the two-sided standardized asymptotic 95% CI for the difference in seroconversion rates between the two study groups (MMRV minus MMR+V) was above .10% for each of the vaccine antigens. A sample size of 474 subjects (MMRV, 316; MMR+V, 158), accounting for a 20% drop-out rate was planned, which gave a power of at least 90% to meet the primary objective.
The analysis of immunogenicity was performed on the according-to-protocol (ATP) cohort. The ATP cohort included all subjects for whom pre- and post-vaccination serology results were available, who were seronegative for at least one vaccine antigen, and who complied with study procedures. Seroconversion rates and geometric mean titers (GMTs) were calculated with exact 95% CIs for antibodies against each vaccine antigen using Proc StatXact [20]. Seroconversion was defined as the appearance of antibodies (i.e., antibody concentration/titer≥cut-off value) in the serum of subjects who were seronegative before vaccination. The 95% CIs for the GMTs were obtained by exponential transformation of the 95% CI for the mean of log-transformed titer.
Analysis of safety was performed on the total vaccinated cohort (TVC) which included all vaccinated subjects. The individual solicited local and general symptoms reported for the subjects during the post-vaccination follow-up period (4-day for local and 43-day for general solicited symptoms) were calculated with exact 95% CIs. Fever reported for the subjects during the 15-day and 43-day follow-up period was calculated with exact 95% CIs. p<0.05 for groups differences in fever were considered statistically significant. Unsolicited symptoms reported during the 43-day post-vaccination follow-up period were recorded with 95% CI. All the SAEs reported during the entire conduct of the study were also recorded.
Results
Demographics
A total of 474 subjects were enrolled in the study (MMRV, 313; MMR+V, 161). Among these, 458 subjects were included in the ATP cohort for immunogenicity (MMRV, 301; MMR+V, 157). The reasons for exclusion from the ATP cohort are provided in Fig. 1. The median age of the subjects in the TVC was 12 months (range, 11 to 23 months); and 57% were male. The study population was predominantly of East Asian heritage (99.6%). The demographic profiles of the two study groups were comparable.
Immunogenicity
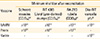
The seroconversion rates and GMTs to the vaccine antigens for MMRV and MMR+V are presented in Table 2. The primary objective of non-inferiority was met for anti-measles, antirubella and anti-varicella antibodies as the lower limit of the 95% CI for the group difference between MMRV and MMR+V groups in terms of seroconversion rates 43 days post-vaccination was greater than the pre-specified cut-off (-10%) (Table 2). However, the lower limit of the 95% CI for the difference in anti-mumps seroconversion rates was lower (-10.40%) than the pre-specified cut-off (-10%) and therefore non-inferiority in terms of anti-mumps seroconversion rate was not met.
Despite failure to meet the non-inferiority criterion, anti-mumps GMTs were comparable between the MMRV (1,012.3; 95% CI, 894.4 to 1,145.7) and MMR+V (934.3; 95% CI, 805.2 to 1,084.1) groups. In addition, the distribution of antibody titers following immunization with MMRV or MMR+V was similar as indicated by the overall shape of the anti-mumps antibody reverse cumulative curve (Fig. 2). Indeed, in a post-hoc analysis using a PRN assay, seroconversion rates for anti-mumps antibodies were 94.3% (95% CI, 91.0 to 96.7) in the MMRV group and 94.0% (95% CI, 88.8 to 97.2) in the MMR+V group, and indicated an anti-mumps seroconversion rate group difference of 0.39 % with a 95% CI lower limit of -4.03% (Table 2).
Safety and reactogenicity
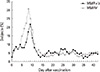
The incidence of solicited local and general symptoms reported within the 4-day and 43-day post-vaccination period in the two groups is presented in Tables 3 and 4. Injection site redness was the most frequently reported solicited local symptom in the MMRV (8.4%; 95% CI, 5.6 to 12.0) and MMR+V (13.2%; 95% CI, 8.4 to 19.5) groups. No grade 3 pain or swelling was reported in either of the groups; grade 3 redness was reported in one subject (0.6%; 95% CI, 0.0 to 3.5) in the MMR+V group. Fever was the most commonly reported solicited general symptom during the 43-day follow-up period in both groups (Table 4). The observed incidence of fever during the 15-day follow-up period was higher in the MMRV group than in the MMR+V group with a peak in the prevalence of fever between day 5 and day 12 post-vaccination (p<0.0001) (Fig. 3). Similarly, the observed incidence of fever was higher in the MMRV group than in the MMR+V group during the 43-day follow-up period (p<0.0052).
Febrile convulsion was reported in two subjects during the 43-day post-vaccination period (days 7 and 20) in the MMRV group. These were considered not related to vaccination by the investigator. Both cases were accompanied by concurrent infection-bronchopneumonia in one case; and bronchopneumonia and pharyngotonsillitis in the other case.
At least one unsolicited symptom was reported for 62.0% (95% CI, 56.4 to 67.4) and 54.7% (95% CI, 46.6 to 62.5) of MMRV and MMR+V recipients, respectively. Among the unsolicited symptoms, upper respiratory tract infection was the most commonly reported symptom in 20.1% (95% CI, 15.8 to 25.0) and 15.5% (95% CI, 10.3 to 22.1) of subjects in the MMRV and MMR+V groups, respectively, during the 43-day post-vaccination follow-up period.
One or more SAEs were reported in 37 subjects (MMRV, 25 out of 310, 8.1%; MMR+V, 12 out of 157, 7.6%). Gastroenteritis was the most commonly reported SAE reported for six subjects in the MMRV group and six subjects in the MMR+V group. Bronchopneumonia was reported for six subjects in the MMRV group and three subjects in the MMR+V group. One SAE related to vaccination was reported. One subject in the MMRV group developed a fever four days post-vaccination and was hospitalized for three days, with a highest reported temperature of 38.8℃. Other SAEs were resolved without sequelae, except one (exacerbation of asthma) which resolved with sequelae in one subject.
Discussion
This study evaluated the safety and immunogenicity of a combined MMRV vaccine compared to co-administrations of MMR and varicella vaccines as separate injections in healthy Korean children during their second year of life. The results demonstrated that MMRV elicited immune responses to measles, rubella and varicella that were non-inferior to that elicited by co-administered MMR and varicella vaccines. The pre-specified non-inferiority criterion was not met for mumps; the lower limit of the 95% CI for the difference in anti-mumps seroconversion rates was marginally lower (-10.40%) than the clinically defined cut-off (-10%).
Despite not having met the non-inferiority criterion, the anti-mumps antibody GMTs observed in the two treatment groups were comparable as indicated by the distribution patterns in the reverse cumulative curve. These findings suggest no substantial difference in the response to mumps, following administration of either MMRV or MMR+V vaccines. Nevertheless, given the difference in anti-mumps seroconversion rates measured by ELISA following vaccination with MMRV as compared to MMR+V, further assessments for anti-mumps immune responses were carried out in a post-hoc analysis using a PRN assay. The anti-mumps seroconversion rates based on the mumps PRN (MMRV 94.3% vs. MMR+V 94.0%) indicated a group difference with a 95% CI lower limit of -4.03%. These results indicated the comparability of immune responses to mumps elicited by MMRV and MMR+V vaccines. Schuster et al reported similar results in a previous clinical study conducted in German subjects aged 10-21 months, where the immune response rates to mumps assessed by the PRN assay (MMRV 96.1% vs. MMR+V 93.6%) indicated a seroconversion rate group difference with a 95% CI lower limit of -7.14 [16].
Unlike other viral infections for which cut-offs for antibody titers in immunoassays are claimed measures of protection against the disease, there is no established correlate of protection for mumps [19]. The advantage of using ELISA is that it measures a broader range of antibody titers than possible with virus neutralization assays. However, ELISA may not detect low levels of antibodies given that it requires initial serum dilutions as high as 1:100. Furthermore, ELISA does not differentiate between neutralizing and non-neutralizing antibodies; as a result of which ELISA may show false-positive results while assessing surrogate markers of protective immune response [19]. This drawback is relevant in the assessment of immune response against mumps, considering mumps virus-specific antibody titers are usually low (less than or equal to 1:8 serum dilutions) in contrast to antibody levels induced by other viruses; mumps virus-neutralizing antibodies are the most reliable surrogate marker of protective immune response [19]. Hence, the PRN assay, with its inherent sensitivity and specificity is considered the gold standard for measuring anti-mumps antibodies [19]. Although a post-hoc analysis, the PRN assay results suggest that the development of protective antibodies to mumps is comparable between the MMR+V and MMRV groups.
In this study, the safety profiles were comparable between the two treatment groups with the exception of fever observed in MMRV recipients. A higher incidence of fever of any grade in the MMRV group when compared to the MMR+V group during the 15-day and 43-day follow-up is in line with the results observed in previous studies [9,21]. These results are comparable with a peak in fever described following administration of other measles-containing vaccines [21]. Similar results were reported by Shinefield et al. in subjects aged 12-23 months with other measles-containing vaccines [22]. In this previous study, during days 5 to 12, subjects vaccinated with one dose of the MMRV vaccine, Proquad (Merck and Co. Inc., Whitehouse Station, NJ, USA) had significantly higher rates of elevated temperatures than subjects co-administered with MMR+V vaccines, M-M-R II and Varivax (both are manufactured by Merck and Co. Inc.) [22]. The results of the current study indicate that a combined MMRV vaccine may be a good candidate for use in national immunization programs [11,23]. Usage of a combined MMRV vaccine is likely to improve the existing MMR immunization coverage rates by facilitating the introduction of varicella vaccines into national immunization schedules and thereby achieving favorable cost-effectiveness [24]. In addition, a combined MMRV vaccine reduces the number of injections, simplifies immunization schedules and improves record keeping [25,26]. Despite these potential benefits, there are concerns with the combined MMRV vaccine. Two post-licensure studies evaluating Proquad (Merck and Co. Inc.) demonstrated an increased incidence in fever and increased risk of febrile convulsions in MMRV recipients compared to MMR+V recipients, post-dose-1 [27,28]. As indicated earlier, increased incidence of fever post-dose-1 in MMRV recipients was observed in the present study as well. Based on these concerns, the American Academy of Pediatrics recommends the administration of either a combined MMRV or separate administrations of MMR and varicella vaccines for the first dose to children aged 12-47 months of age [29]. In addition, they recommend that providers considering administration of combined MMRV should discuss the benefits and risks of both vaccination options with parents/caregivers [29]. In cases where providers are unable to clearly communicate the benefits and risks, the option of MMR and varicella vaccines should be considered [29].
In conclusion, the results of the present study demonstrated non-inferiority of the MMRV vaccine compared to co-administration of MMR+V vaccines for all antigens except mumps, based on the pre-specified non-inferiority criterion. Comparable immune responses were elicited by MMRV and MMR+V on a post-hoc analysis using the PRN assay. Furthermore, an acceptable safety profile was indicated, except for a higher incidence of fever following the MMRV vaccination. Despite the higher rate of fever and considering the potential benefits, the inclusion of the combined MMRV vaccine in national immunization programs offers the potential to improve varicella uptake in several countries.





 XML Download
XML Download