

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Influenza viruses have been the cause of morbidity and mortality in both animals and humans [1,2,3]. Since the first emergence in Mexico, the 2009 pandemic A (H1N1) virus has been circulating worldwide as a form of seasonal influenza virus up to date [4,5]. Accordingly, it is reported that influenza A (H1N1)-pdm09 is the most commonly detected virus in most areas of the southern hemisphere. However, influenza virus subtypes vary considerably from country to country [6,7]. Although, ongoing incidence of the H7N9 avian influenza infections occurs in China, still no evidence of any sustained human-to-human transmission has been reported [8].
As a preparedness for future influenza virus pandemic, vaccine development might be considered as the most effective and essential strategy [9,10]. For the development of successful vaccine for influenza, vaccine industry may need development of adjuvants that allows cheaper and more effective vaccine production. During the past decade, a large number of novel adjuvants have been developed and evaluated clinically [11]. There are several adjuvanted influenza vaccines that have been licensed for use in human. Currently, MF59 (Novartis Vaccines and Diagnostics) and aluminum hydroxide (alum) are the two main adjuvants that used largely for production of influenza vaccines [12,13,14]. The adjuvant MF59 has been shown to have a robust safety and efficacy profiles with inducing cross-reactive antibodies against influenza viruses [15], since it was approved for human use more than a decade ago as a type of oil-emulsion adjuvant [14,15,16].
New vaccine adjuvant and vaccine delivery systems have been developed experimentally over the past few years. Among them, we have developed a promising adjuvant candidate called mOMV which is modified outer membrane vesicles (mOMVs). OMVs are considered as an attractive vaccine adjuvant and antigen delivery platform since they were proven to be effective in human meningococcal vaccine and other experimental vaccines in several countries [17,18]. It is known that wild-type OMV (wOMV) has intrinsic inflammatory potential due to their composition with bacterial cell wall constituents such as lipopolysaccharide (LPS) and peptidoglycan [19]. However, the LPS-modified OMV with strictly penta-acylated lipid A can be produced from Escherichia coli mutant, in order to reduce potential side-effects of the OMV, due to endotoxin activity of its LPS component. Hence, this newly-produced mOMV would be much less-endotoxic and safer than wOMV [19].
Both alum and MF59 adjuvants have been very well known and proven to possess immune stimulatory properties in the adjuvanted vaccines against influenza viruses. It is worth comparing for these widely used adjuvants with the mOMV and studying for its adjuvant efficacy against a highly virulent influenza virus. In this study, we investigated the efficacy of mOMV adjuvant in the split vaccine of A/California/04/09 (CA04, H1N1) by using BALB/c mice via the intramuscular route. Vaccination and challenge experiments in this mouse model study demonstrated that mOMV has a sufficient adjuvant effect on inducing protection from the lethal challenge with influenza A/California/04/09 (maCA04, H1N1) virus. In addition, the H1N1 split vaccine mixed with the combined adjuvant (mOMV plus alum) was more effective in the protection of mice than that of mOMV or alum alone group against challenge with maCA04 (H1N1) virus.
Materials and Methods
Vaccine preparation
A/California/04/09 (CA04, H1N1) split vaccine antigen was kindly provided by The Green Cross Reference Lab (Yongin, Korea). Mouse-adapted influenza A/California/04/09 (maCA04, H1N1) virus was generated by site-directed mutagenesis using the GeneTailor kit (Invitrogen, Carlsbad, CA, USA) according to the manufacturer's instructions. Briefly, the positions at 12, 58, and 88 in PB1-F2 stop codons, which are required for PB1-F2 protein expression, were mutated to serine (S), tryptophan (T), and tryptophan (T), respectively. In addition, the previously known PA (T97I) mutant was also incorporated to enhance virulence in mice [20]. The resulting maCA04 (H1N1) virus was propagated in 11-day-old-embryonic eggs at 37℃ for 72 hours. The allantoic fluid containing the virus was harvested and centrifuged to remove unwanted debris at 3,000 rpm for 10 minutes at 4℃. The harvested virus was dispensed in aliquots and stored at -80℃ until further use. Virus titers were calculated as previously described [20,21].
Vaccination and virus challenge experiments
Four-week-old BALB/c female mice were purchased from Samtako (Osan, Korea). Groups of mice (10 animals per group) were intramuscularly vaccinated with the split vaccine containing 0.05, 0.1, and 0.5 µg/dose of hemagglutinin (HA), respectively, that were mixed with alum (vaccine-alum), MF59 (vaccine-MF59), mOMV (vaccine-mOMV), and the combined adjuvant (vaccine-mOMV plus alum) in 0.2 mL of sterile phosphate-buffered saline (PBS) with two doses at two week intervals, respectively. Two weeks after the last immunization, mice were intranasally (i.n.) challenged with 10 times 50% tissue culture infective doses (TCID50) of the A/California/04/09 (maCA04 [H1N1]) virus. The control group received adjuvant only in 0.25 mL of sterile PBS.
Cell line and hemagglutination inhibition test
Madin-Darby Canine Kidney (MDCK) cells cultured in Eagle's minimal essential medium (EMEM; GIBCO-BRL, Bethesda, MD, USA) with 5% fetal bovine serum (LONZA Inc., Basel, Switzerland), 1% penicillin/streptomycin (Gibco-Invitrogen Inc., Carlsbad, CA, USA), and 1% non-essential amino acids (Gibco-Invitrogen Inc). Cultured MDCK cells were split into 1×105 cells per well in a 96-well plate. Hemagglutination inhibition (HI) assays were done with collected mice sera. Mice sera were collected 2 weeks after each vaccine administration and stored at -80℃ until use. Briefly, the mice sera were treated with receptor destroying enzyme (RDE; Denka Seiken, Tokyo, Japan) to inactivate non-specific inhibitors with a final serum dilution of 1:10. RDE-treated sera were serially diluted 2-fold and 100 TCID50/mL of virus was added to each well. The plates were incubated at room temperature for 30 minutes followed by the addition of 0.5% turkey red blood cells (tRBCs). The plates were incubated at 37℃ for 30 minutes. The HI titer was determined by the reciprocal of the last dilution that contained tRBCs with no agglutination. The limit of detection for the HI assays done was set to ≤20 HI units.
Vaccine experiment and virus titers in lung tissues
The body weight and survival rate was measured daily on days 1 through 15 after challenge virus inoculation. Lung samples from two mice per groups were collected at 1, 3, 5, 7 and 9 days post-infection (dpi) and homogenized with equal volumes (1 mL/g tissue) of PBS-containing 10% antibiotics. Tissue homogenates were clarified by centrifugation at 12,000× rpm for 10 minutes at 4℃ and then supernatants were transferred to new tubes. Samples were 10-fold serially diluted immediately after collection and then inoculated into MDCK cells seeded in 96-well plate plates for virus titration. The plates were incubated at the 37℃ CO2 incubator for 2 hours for viral absorbency. Inoculated supernatant was removed and replaced with EMEM containing 1 µg/mL TPCK-trypsin and then incubated at 37℃ for 48 hours. Virus cytopathic effect was observed daily and the viral titer was determined by the HA test. Hemagglutination assay was performed after 48 hours using tRBCs.
Statistical analysis
Statistical significance of differences in quantitative virus was compared between each vaccinated group and analyzed using the unpaired Student's t test (two-tailed). The value, p<0.05 considered statistically significant was used to determine the p-values of survival calculated by the GraphPad Prism version 5.0 for Window (GraphPad Software, LA Jolla, CA, USA).
Results
Antibody response induced by mouse vaccination
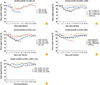
To investigate the adjuvant efficacy, mice sera from vaccinated groups were analyzed by HI assay to identify IgG antibodies raised against influenza virus. All booster vaccinated groups received the H1N1 split vaccine could elicit the detectable HI titers (≥20 HI unit) against the virus, but no detectable HI titer was observed in the first vaccination and the adjuvant only control groups (Fig. 1). In particular, high HI titer was detected from the 0.5 µg/dose of CA04 (H1N1) split vaccine-MF59 (39 HI), -alum (38 HI), and -mOMV (23 HI) adjuvant groups in the booster vaccine groups, respectively (Fig. 1B, 1C, and 1D), while the split antigen only group showed the lowest HI titers (≤20 HI) against the virus (maCA04 [H1N1]). However, there was no detectable mean HI titer against the heterologous influenza A/Perth/16/2009 (H3N2) and A/PR8/8/34 (H1N1) virus in the vaccinated groups (data not shown).Notably, although it is not statistically significant, the vaccinated group received 0.05 µg/dose of HA in the vaccine-mOMV plus alum could induce a similar level of HI titer comparable to that of the vaccine groups received 0.1 or 0.5 µg/dose of HA (p=0.0695 or p=0.087, respectively). However, when the sera were obtained from the first vaccinated mice with the vaccine-mOMV plus alum, only basal mean HI titer was detected (≤20 HI). Taken together, booster vaccination with the split vaccine-mOMV could efficiently raise HI titer against maCA04 (H1N1) virus.
Survival rate and body weight change after challenge in vivo
Two weeks after last vaccination, all vaccinated groups of mice were challenged i.n. with 10 times 50% mouse lethal dose (MLD50) of A/California/04/09 (maCA04, H1N1) virus. To assessthe protective efficacy played by mOMV adjuvant, vaccinated mice received the vaccine-mOMV adjuvant was monitored for the survival rate and body weight change, compared with the cases of vaccine-MF59, -alum, and the vaccine-mOMV plus alum groups (Fig. 2). All mice boosted with 0.1 and 0.5 µg/dose of the adjuvanted vaccine groups could induce high survival rate to 80% and 100% at 15 post day infection (dpi), respectively. However, mock-vaccinated mice, the adjuvant only group, and the mice received 0.05 µg/dose of the antigen alone showed gradual body weight loss and all succumbed to virus challenge within 7 or 8 dpi with severe clinical signs (Figs. 2, 3). On the other hand, it is noteworthy that the mice received 0.05 µg/dose of the vaccine-mOMV plus alum showed attenuation of body weight loss, extended survival, and complete protection, likely those observed in the cases with 0.1 and 0.5 µg/dose of the vaccine during the course of the experiment (Figs. 2E, 3E). In contrast, a significantly reduced mortality was exhibited in the vaccinated mice received 0.05 µg/dose of the vaccine containing 10 µg of mOMV (40%), alum (50%), and MF59 (60%). The antigen only group also showed a gradual body weight loss and succumbed at 7 dpi in the 0.05 µg/dose group. The vaccinated mice received 0.1 and 0.5 µg/dose of HA survived only 20% and 30% at 15 dpi, respectively. Taken together, these results suggest that the vaccine-mOMV has a capacity similar or same protective efficacy to the vaccine-alum or -MF59. Furthermore, the vaccine-mOMV plus alum at 0.05 µg/dose of HA could induce a better protection than the single mOMV adjuvanted vaccine against lethal challenge with maCA04 (H1N1) virus.
Viral load in the lung of vaccinated mice
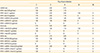
To determine the viral load in the lung of vaccinated mice, virus titers of each group were monitored (Table 1). Viral titers in the mice lung (collected at 2, 4, 6, 8, and 10 dpi) showed that the vaccine-mOMV group efficiently inhibited viral replication at 4 and 6 dpi upon lethal challenge with maCA04 (H1N1) virus, compared to the mock (adjuvant and antigen only) groups (Table 1). Viral titers in the vaccine-mOMV group at 0.5 µg/dose showed similar levels of virus titer with those groups received the vaccine-alum and -MF59 adjuvants. As expected, adjuvant alone groups exhibited a clear increase of virus replication in the lungs ranging from 2.50 to 3.75 TCID50 titration (log10TCID50/mL) from 2 to 6 dpi. All the adjuvanted vaccine groups at 0.1 µg/dose of HA appeared to inhibit virus replication in the mice lung, compared to the antigen only group. However, viral inhibition was not detected at the 0.05 µg/dose of the vaccine-MF59 and similar or gradual viral inhibition was detected at the 0.05 µg/dose of the vaccine-mOMV, -alum after 6 and 8 dpi, respectively. Although, it is not statically significant, it is noteworthy that the vaccine-mOMV plus alum at 0.05 µg/dose of HA could clearly induce the most efficient inhibition of lung viral titers starting at 6 dpi with 1.25 TCID50. We demonstrated that the H1N1 vaccine-mOMV could elicit the strong immune response enough to clear the viral load in the infected lung of the vaccinated mice. Altogether, these results clearly demonstrated that mOMV can exert the adjuvant effect by itself and showed synergistic effects when it mixed with alum. Consequently, mOMV could be used as a next-generation vaccine adjuvant for production of a cheaper and more effective vaccines developed as a mean of preparedness to influenza virus pandemic in the future.
Discussion
Now a days, MF59 is the most commonly used adjuvant for influenza virus vaccines. The squalene oil-in-water emulsion (MF59) provides immunogenicity and protection against influenza virus in humans. However, despite the effectiveness, intricate process in manufacturing and higher production cost would be still a matter of concern for MF59 to be accepted as next generation vaccine adjuvant.
The mOMV we developed previously is a novel, nano-size particle, generated from the ΔmsbB/ΔpagP mutant of non-pathogenic E. coli W3110 and thus very cost effective, compared with other adjuvants. In this study, we compared the adjuvant efficacy of the mOMV with that of well-known adjuvants such as MF59 and alum by using H1N1-pdm09 split vaccine. We demonstrated that the vaccine-mOMV could induce a protective immunity when evaluated by survival rate and body weight loss due to the adjuvant efficacy for inducing high HI titers against maCA04 (H1N1) virus, compared to the antigen only or the adjuvant only groups.
A number of studies with a view to assessing adjuvant efficacy have been conducted with accumulation of safety profiles [22,23]. MF59 adjuvant was effective in inducing immunogenicity of the vaccine approximately 3 times higher than the case of alum-adjuvanted vaccine [24], in agreement with the previous study in hepatitis B virus vaccines [25]. Also, the results obtained from this study using the booster vaccinated mice received the adjuvanted vaccines could induce high mean HI titer and protect efficiently from lethal challenge with maCA04 (H1N1) virus, although the first inoculated mice groups could not elaborate high HI titers. The mOMV-adjuvanted vaccine elaborated viral clearance against maCA04 (H1N1) in the mice lung. This result clearly demonstrated that mOMV adjuvant plays an important role in the efficacy of influenza vaccine by inducing high mean HI titer and protecting the lung from viral replication (Table 1, Fig. 1).
Previous studies indicated that inactivated 2009 H1N1 influenza vaccine at varying dosages of HA with extemporaneously mixed AS03 adjuvant system was improved the immune response at high dosage adjuvant vaccine on adult groups [26]. In agreement with these results, we demonstrated that 0.05 µg/dose of HA containing mixed with mOMV and alumadjuvant attenuated body weight loss and increased survival rate after challenge maCA04 (H1N1) virus infection than those of individual adjuvant groups. Those results might be due to the possibility that the combined adjuvant (mOMV plus alum) have played synergistically in the vaccine. The mOMV has adjuvant activity on T cell priming in a Toll-like receptor 4 (TLR4)-dependent manner [19,27]. Furthermore, mOMV can stimulate DCs enough to up-regulate expression of co-stimulatory and antigen-presenting molecules and to produce proinflammatory cytokines in a TLR-dependent fashion [19].
In summary, our results suggest that mOMV can exert not only the self-adjuvanticity but also a synergy effect for influenza vaccine efficacy when combined with alum. Thus, mOMV could be used as a vaccine platform for development of various formulations to prepare future influenza pandemic.


 XML Download
XML Download