

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Hyeong Woo Kim, Yong Sun Choi, Jung Ho Won, Jae Min Lee, Jin Young Heo, Jung Ah Choi, Mi-Jung Oh
Abstract
Acute generalized exanthematous pustulosis (AGEP) is a severe and rare disease usually related to drug eruption. AGEP is induced by drugs in over 90% of cases with antibiotics being the most common. It is characterized by a fever and a pustular eruption on erythematous skin with acute onset and without follicular localization. Acetaminophen is commonly used as an antipyretic and analgesic. Acetaminophen has been reported to be an uncommon cause of AGEP. We report a 79-year-old woman presenting with fever and erythematous maculopapular eruptions on the trunk with sterile pustules arising upon the use of acetaminophen for back pain. Leukocytosis and elevated C-reactive protein levels were noted on the laboratory examination. The histopathological examination of the skin biopsy specimen showed intraepidermal pustule formation with superficial perivascular lymphocytic infiltration, including eosinophils, and extensive red blood cell extravasation. The lesions were resolved with discontinuation of acetaminophen and use of systemic corticosteroid. We report a case of AGEP probably caused by acetaminophen.
Figures and Tables
Fig. 1
There are multiple nonfollicular, pustular lesions on an erythematous background on the back.


Fig. 3
Histologic examination shows intraepidermal pustule formation with superficial perivascular lymphocytic infiltration including eosinophils and extensive red blood cell extravasation (A: H&E, ×100; B: H&E, ×200).
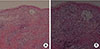
Table 1
Scores for the diagnosis of AGEP (proposed by the EuroSCAR group)2

AGEP, acute generalized exanthematous pustulosis.
Interpretationn (score): 0, not AGEP; 1–4, AGEP is possible; 5–7, AGEP is probable; 8–12, AGEP is established.
*Typical: typical morphology. †Compatible: morphology is not typical but strongly suggestive. ‡Insufficient: lesions cannot be evaluated (due to advanced stage of development).
Adapted from Sidoroff et al. J Cutan Pathol 2001;28:113-9, with permission of John Wiley and Sons.2
References
1. Bomarrito L, Zisa G, Delrosso G, Farinelli P, Galimberti M. A case of acute generalized exanthematous pustulosis due to amoxicillin-clavulanate with multiple positivity to beta-lactam patch testing. Eur Ann Allergy Clin Immunol. 2013; 45:178–180.
2. Sidoroff A, Halevy S, Bavinck JN, Vaillant L, Roujeau JC. Acute generalized exanthematous pustulosis (AGEP): a clinical reaction pattern. J Cutan Pathol. 2001; 28:113–119.

3. Brockow K, Garvey LH, Aberer W, Atanaskovic-Markovic M, Barbaud A, Bilo MB, et al. Skin test concentrations for systemically administered drugs: an ENDA/EAACI Drug Allergy Interest Group position paper. Allergy. 2013; 68:702–712.
4. Mashiah J, Brenner S. A systemic reaction to patch testing for the evaluation of acute generalized exanthematous pustulosis. Arch Dermatol. 2003; 139:1181–1183.
5. Romano A, Viola M, Gaeta F, Rumi G, Maggioletti M. Patch testing in non-immediate drug eruptions. Allergy Asthma Clin Immunol. 2008; 4:66–74.
6. Bachot N, Roujeau JC. Differential diagnosis of severe cutaneous drug eruptions. Am J Clin Dermatol. 2003; 4:561–572.
7. Sidoroff A, Dunant A, Viboud C, Halevy S, Bavinck JN, Naldi L, et al. Risk factors for acute generalized exanthematous pustulosis (AGEP)-results of a multinational case-control study (EuroSCAR). Br J Dermatol. 2007; 157:989–996.
8. Britschgi M, Steiner UC, Schmid S, Depta JP, Senti G, Bircher A, et al. T-cell involvement in drug-induced acute generalized exanthematous pustulosis. J Clin Invest. 2001; 107:1433–1441.
9. Kardaun SH, Kuiper H, Fidler V, Jonkman MF. The histopathological spectrum of acute generalized exanthematous pustulosis (AGEP) and its differentiation from generalized pustular psoriasis. J Cutan Pathol. 2010; 37:1220–1229.
10. Sener O, Kose Ö, Kartal Ö, Safali M. Acute generalized exanthematous pustulosis due to oral use of blue dyes. Korean J Intern Med. 2011; 26:360–363.
11. Szatkowski J, Schwartz RA. Acute generalized exanthematous pustulosis (AGEP): a review and update. J Am Acad Dermatol. 2015; 73:843–848.
12. Wolkenstein P, Chosidow O, Fléchet ML, Robbiola O, Paul M, Dumé L, et al. Patch testing in severe cutaneous adverse drug reactions, including Stevens-Johnson syndrome and toxic epidermal necrolysis. Contact Dermatitis. 1996; 35:234–236.
13. Halevy S, Cohen A, Livni E. Acute generalized exanthematous pustulosis associated with polysensitivity to paracetamol and bromhexine: the diagnostic role of in vitro interferon-gamma release test. Clin Exp Dermatol. 2000; 25:652–654.
 XML Download
XML Download