

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Sun Hee Choi1, Dae Jin Song2, Hye Yung Yum3, Yong Mean Park4, Yeong Ho Rha1
Abstract
Cough is one of the common symptoms, which is usually related to respiratory infections for children. This symptom is not considered crucial. Published data reported that the community prevalence of chronic cough in primary school children is 5%–10%, while the prevalence is likely to be higher in younger children. The cause of persistent cough should be investigated. There were significant differences in the causes and management for cough according to age. Chronic cough is defined as duration of 4 weeks or longer. Common culprits for chronic cough in children are different from those in adults. The authors reviewed articles about chronic cough of children to help improve the understanding and management for pediatric chronic cough.
Figures and Tables
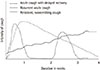 | Fig. 1The different patterns of cough according to duration and severity. Adapted from Marais BJ, et al. Arch Dis Child 2005;90:1162-5,with permission of the BMJ Publishing Group Ltd.6
|
 | Fig. 2Classification of types of cough in children. Adapted from Chang AB, et al. Chest 2006;129(1 Suppl):260S-283S, with permission of the Elsevier.2
|
 | Fig. 3Pathophysiology of cough reflex. Reprinted from Korean Academy of Pediatric Allergy and Respiratory Disease. Pediatric allergy immunology pulmonology. 2nd ed. Seoul: Ryo Moon Gak.P.Co., 2013, with permission of Korean Academy of Pediatric Allergy and Respiratory Disease.7
|
 | Fig. 4Representative scheme of afferent and efferent pathways that regulate cough, and of the pathophysiology of the enhanced cough reflex. RAR, rapidly adapting receptor; SAR, slowly adapting fibres; NTS, nucleus tractus solitarius; CGRP, calcitonin gene-related peptide; LTD4, leukotriene D4; PGE2, prostaglandin E; NK1, neulokinin-1; TRPV, transient receptor potential vanilloid; TNF, tumour necrosis factor. Adapted from Chung KF, et al. Lancet 2008;371:1364-74, with permission of the Elsevier.10
|
 | Fig. 5Approach to pediatric chronic cough. BDR, bronchodilator response; BHR, bronchial hyperresponsiveness; HRCT, high resolution computed tomography; PND, postnasal discharge; PNS, paranasal sinus; dz, diseases; Bx, biopsy; CT, computed tomography; TB, tuberculosis.
|
 | Fig. 6The approach to a child with nonspecific chronic cough. Modified from Chang AB, Paediatr Child Health 2008;18:333-9, with permission of the Elsevier.64
|
Table 1
Pointers suggesting specific cough

![]()
Table 2
Etiologic factors of chronic cough in children, including differences from adults and level of evidence defining cause and effect

Modified from Chang AB, et al. Otolayngol Clin N Am 2010;43:181-98, with permission of the Elsevier.34
FEV1, forced expiratory volume in 1 second; PCR, polymerase chain reaction; CF, cystic fibrosis; CT, computed tomography; GERD, gastroesophageal reflux disease.
![]()
Table 3
Summary of therapies use for cough in children as reported in literatures based on controlled trials

AE, adverse events; CS, corticosteroids; LTRA, leukotriene receptor antagonists; NR, not relevant; OTC, over-the-counter; PPI, proton pump inhibitors; RCT, randomised controlled trials.
Modified from Chang AB, et al. Otolayngol Clin N Am 2010;43:181-98, with permission of the Elsevier.34
![]()
References
1. Chang AB, Landau LI, Van Asperen PP, Glasgow NJ, Robertson CF, Marchant JM, et al. Cough in children: definitions and clinical evaluation. Med J Aust. 2006; 184:398–403.

2. Chang AB, Glomb WB. Guidelines for evaluating chronic cough in pediatrics: ACCP evidence-based clinical practice guidelines. Chest. 2006; 129:1 Suppl. 260S–283S.
3. Chang AB. Cough. Pediatr Clin North Am. 2009; 56:19–31. ix
4. Cho B, Lee JS, Hwang KT, Cho SH. Chronic cough in children. J Korean Pediatr Soc. 1994; 37:1116–1123.
5. Shields MD, Bush A, Everard ML, McKenzie S, Primhak R. British Thoracic Society Cough Guideline Group. BTS guidelines: recommendations for the assessment and management of cough in children. Thorax. 2008; 63:Suppl 3. iii1–iii15.
6. Marais BJ, Gie RP, Obihara CC, Hesseling AC, Schaaf HS, Beyers N. Well defined symptoms are of value in the diagnosis of childhood pulmonary tuberculosis. Arch Dis Child. 2005; 90:1162–1165.
7. Korean Academy of Pediatric Allergy and Respiratory Disease. Pediatric allergy immunology pulmonology. 2nd ed. Seoul: Ryo Moon Gak.P.Co.;2013.
8. Widdicombe J, Fontana G. Cough: what's in a name? Eur Respir J. 2006; 28:10–15.
9. Committee for the Japanese Respiratory Society Guidelines for Management of Cough. Kohno S, Ishida T, Uchida Y, Kishimoto H, Sasaki H, et al. The Japanese Respiratory Society guidelines for management of cough. Respirology. 2006; 11:Suppl 4. S135–S186.
10. Chung KF, Pavord ID. Prevalence, pathogenesis, and causes of chronic cough. Lancet. 2008; 371:1364–1374.
11. Widdicombe J. The race to explore the pathway to cough: who won the silver medal? Am J Respir Crit Care Med. 2001; 164:729–730.
12. Bonham AC, Sekizawa SI, Joad JP. Plasticity of central mechanisms for cough. Pulm Pharmacol Ther. 2004; 17:453–457.
13. Chang AB, Gibson PG, Ardill J, McGarvey LP. Calcitonin gene-related peptide relates to cough sensitivity in children with chronic cough. Eur Respir J. 2007; 30:66–72.
14. Chang AB, Phelan PD, Sawyer SM, Robertson CF. Airway hyperresponsiveness and cough-receptor sensitivity in children with recurrent cough. Am J Respir Crit Care Med. 1997; 155:1935–1939.
15. Chang AB, Redding GJ, Everard ML. Chronic wet cough: protracted bronchitis, chronic suppurative lung disease and bronchiectasis. Pediatr Pulmonol. 2008; 43:519–531.
16. Wood RE. Localized tracheomalacia or bronchomalacia in children with intractable cough. J Pediatr. 1990; 116:404–406.
17. Gormley PK, Colreavy MP, Patil N, Woods AE. Congenital vascular anomalies and persistent respiratory symptoms in children. Int J Pediatr Otorhinolaryngol. 1999; 51:23–31.
18. Gay M, Blager F, Bartsch K, Emery CF, Rosenstiel-Gross AK, Spears J. Psychogenic habit cough: review and case reports. J Clin Psychiatry. 1987; 48:483–486.
19. Butani L, O'Connell EJ. Functional respiratory disorders. Ann Allergy Asthma Immunol. 1997; 79:91–99.
20. Grüber C, Lehmann C, Weiss C, Niggemann B. Somatoform respiratory disorders in children and adolescents-proposals for a practical approach to definition and classification. Pediatr Pulmonol. 2012; 47:199–205.
21. Harnden A, Grant C, Harrison T, Perera R, Brueggemann AB, Mayon-White R, et al. Whooping cough in school age children with persistent cough: prospective cohort study in primary care. BMJ. 2006; 333:174–177.
22. Schaad UB, Rossi E. Infantile chlamydial pneumonia: a review based on 115 cases. Eur J Pediatr. 1982; 138:105–109.
23. Phelan PD, Landau LI, Olinsky A. Respiratory illness in children. 3rd ed. Oxford: Blackwell Scientific Publications;1990.
24. Jegoux F, Legent F, Beauvillain de Montreuil C. Chronic cough and ear wax. Lancet. 2002; 360:618.
25. Wolff AP, May M, Nuelle D. The tympanic membrane: a source of the cough reflex. JAMA. 1973; 223:1269.
26. Mehdi N, Weinbuerger M, Abu-Hasan M. Etiology and outcome of childhood chronic cough using a simple diagnostic approach. Pediatr Asthma Allergy Immunol. 2005; 18:55–61.
27. Marchant JM, Masters IB, Taylor SM, Cox NC, Seymour GJ, Chang AB. Evaluation and outcome of young children with chronic cough. Chest. 2006; 129:1132–1141.
28. Marchant JM, Morris P, Gaffney JT, Chang AB. Antibiotics for prolonged moist cough in children. Cochrane Database Syst Rev. 2005; (4):CD004822.
29. Chang AB, Upham JW, Masters IB, Redding GR, Gibson PG, Marchant JM, et al. Protracted bacterial bronchitis: the last decade and the road ahead. Pediatr Pulmonol. 2016; 51:225–242.
30. Webb WR, Muller NL, Naidich DP. High-resolution CT of the lung. Philadelphia: Lippincott, Williams & Wilkin;2001.
31. Tiddens HA. Detecting early structural lung damage in cystic fibrosis. Pediatr Pulmonol. 2002; 34:228–231.
32. Lim PJ, Park JO, Lee DH, Shin SM, Kim DW. Gastroesophageal reflux disease in children with chronic cough. J Korean Pediatr Soc. 1998; 41:1234–1242.
33. Asilsoy S, Bayram E, Agin H, Apa H, Can D, Gulle S, et al. Evaluation of chronic cough in children. Chest. 2008; 134:1122–1128.
34. Chang AB, Berkowitz RG. Cough in the pediatric population. Otolaryngol Clin North Am. 2010; 43:181–198. xii
35. McKenzie S. The clinical features and their assessment. In : Silveman M, editor. Childhood asthma and other wheezing disorder. 2nd ed. London: Arnold;2002. p. 106–124.
36. Timonen KL, Pekkanen J, Korppi M, Vahteristo M, Salonen RO. Prevalence and characteristics of children with chronic respiratory symptoms in eastern Finland. Eur Respir J. 1995; 8:1155–1160.
37. Marchant JM, Gibson PG, Grissell TV, Timmins NL, Masters IB, Chang AB. Prospective assessment of protracted bacterial bronchitis: airway inflammation and innate immune activation. Pediatr Pulmonol. 2008; 43:1092–1099.
38. Gedik AH, Cakir E, Torun E, Demir AD, Kucukkoc M, Erenberk U, et al. Evaluation of 563 children with chronic cough accompanied by a new clinical algorithm. Ital J Pediatr. 2015; 41:73.
39. Hay AD, Wilson AD. The natural history of acute cough in children aged 0 to 4 years in primary care: a systematic review. Br J Gen Pract. 2002; 52:401–409.
40. Kusel MM, de Klerk N, Holt PG, Landau LI, Sly PD. Occurrence and management of acute respiratory illnesses in early childhood. J Paediatr Child Health. 2007; 43:139–146.
41. Hallander HO, Gnarpe J, Gnarpe H, Olin P. Bordetella pertussis, Bordetella parapertussis, Mycoplasma pneumoniae, Chlamydia pneumoniae and persistent cough in children. Scand J Infect Dis. 1999; 31:281–286.
42. Braman SS. Postinfectious cough: ACCP evidence-based clinical practice guidelines. Chest. 2006; 129:1 Suppl. 138S–146S.
43. Ministry of Health and Welfare. Centers for Disease Control & Prevention. Korean guidelines for tuberculosis. 2nd ed. Cheongju: Ministry of Health and Welfare;Centers for Disease Control & Prevention;2014.
44. Lombardi E, Stein RT, Wright AL, Morgan WJ, Martinez FD. The relation between physician-diagnosed sinusitis, asthma, and skin test reactivity to allergens in 8-year-old children. Pediatr Pulmonol. 1996; 22:141–146.
45. Turktas I, Dalgic N, Bostanci I, Cengizlier R. Extrathoracic airway responsiveness in children with asthma-like symptoms, including chronic persistent cough. Pediatr Pulmonol. 2002; 34:172–180.
46. Gawchik S, Goldstein S, Prenner B, John A. Relief of cough and nasal symptoms associated with allergic rhinitis by mometasone furoate nasal spray. Ann Allergy Asthma Immunol. 2003; 90:416–421.
47. Usta Guc B, Asilsoy S, Durmaz C. The assessment and management of chronic cough in children according to the British Thoracic Society guidelines: descriptive, prospective, clinical trial. Clin Respir J. 2014; 8:330–337.
48. Goldsobel AB, Chipps BE. Cough in the pediatric population. J Pediatr. 2010; 156:352–358.
49. Yalçin E, Dogru D, Haliloglu M, Ozcelik U, Kiper N, Gocmen A. Postinfectious bronchiolitis obliterans in children: clinical and radiological profile and prognostic factors. Respiration. 2003; 70:371–375.
50. Davies MJ, Fuller P, Picciotto A, McKenzie SA. Persistent nocturnal cough: randomised controlled trial of high dose inhaled corticosteroid. Arch Dis Child. 1999; 81:38–44.
51. van Asperen PP, McKay KO, Mellis CM, Loh RK, Harth SC, Thong YH, et al. A multicentre randomized placebo-controlled double-blind study on the efficacy of Ketotifen in infants with chronic cough or wheeze. J Paediatr Child Health. 1992; 28:442–446.
52. Chang AB, Winter D, Acworth JP. Leukotriene receptor antagonist for prolonged non-specific cough in children. Cochrane Database Syst Rev. 2006; (2):CD005602.
53. Chang AB, McKean M, Morris P. Inhaled anti-cholinergics for prolonged non-specific cough in children. Cochrane Database Syst Rev. 2004; (1):CD004358.
54. Morris PS, Leach AJ. Withdrawn: antibiotics for persistent nasal discharge (rhinosinusitis) in children. Cochrane Database Syst Rev. 2008; (2):CD001094.
55. Morris P, Leach A. Antibiotics for persistent nasal discharge (rhinosinusitis) in children. Cochrane Database Syst Rev. 2002; (4):CD001094.
56. Gottfarb P, Brauner A. Children with persistent cough: outcome with treatment and role of Moraxella catarrhalis? Scand J Infect Dis. 1994; 26:545–551.
57. Chang AB, Peake J, McElrea MS. Anti-histamines for prolonged non-specific cough in children. Cochrane Database Syst Rev. 2006; (3):CD005604.
58. Rudolph CD, Mazur LJ, Liptak GS, Baker RD, Boyle JT, Colletti RB, et al. Guidelines for evaluation and treatment of gastroesophageal reflux in infants and children: recommendations of the North American Society for Pediatric Gastroenterology and Nutrition. J Pediatr Gastroenterol Nutr. 2001; 32:Suppl 2. S1–S31.
59. Chang AB, Lasserson TJ, Gaffney J, Connor FL, Garske LA. Gastro-oesophageal reflux treatment for prolonged non-specific cough in children and adults. Cochrane Database Syst Rev. 2011; (1):CD004823.
60. Orenstein SR, Hassall E, Furmaga-Jablonska W, Atkinson S, Raanan M. Multicenter, double-blind, randomized, placebo-controlled trial assessing the efficacy and safety of proton pump inhibitor lansoprazole in infants with symptoms of gastroesophageal reflux disease. J Pediatr. 2009; 154:514–520.e4.
61. Hovell MF, Zakarian JM, Matt GE, Hofstetter CR, Bernert JT, Pirkle J. Effect of counselling mothers on their children's exposure to environmental tobacco smoke: randomised controlled trial. BMJ. 2000; 321:337–342.
62. Murphy KR. Allergic rhinitis in children: selecting an intranasal corticosteroid. Pediatr Asthma Allergy Immunol. 2005; 18:216–229.
63. Davies MJ, Cane R, Ranganathan S, McKenzie SA. Cough, wheeze and sleep. Arch Dis Child. 1998; 79:465.
64. Chang AB. Chronic non-specific cough in children. Paediatr Child Health. 2008; 18:333–339.
 XML Download
XML Download