

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Jisun Yoon1, Jun-Sung Park1, Hyun-Ju Cho1, Eun Lee1, Song-I Yang2, Soo-Jong Hong1, Jinho Yu1
Abstract
Purpose
Asthma is a chronic airway inflammatory disease characterized by bronchial hyperresponsiveness and reversible airway obstruction. Bronchial challenge with methacholine or adenosine-5'-monophosphate (AMP) has been used to diagnose asthma. Recently, measurement of exhaled nitric oxide (eNO) can also be used for the diagnosis of asthma. The aim of this study was to compare the diagnostic value for asthma between challenge with methacholine or AMP and eNO in children with chronic nonspecific respiratory symptoms.
Methods
One hundred thirty-three children who have chronic nonspecific respiratory symptoms were enrolled. Bronchial challenge with methacholin and AMP were performed, and eNO was measured in all subjects. Subjects were defined as asthma based on the clinical symptoms and bronchodilator response during follow-up of at least 3 months after test.
Results
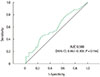
Thirty-three subjects (34%) were finally diagnosed as asthma among 97 patients after 3-month follow-up. The area under the receiver operating characteristic curves for the diagnosis of asthma were 0.903 (95% confidence interval [CI], 0.838-0.969; P<0.001) for methacholline challenge, 0.867 (95% CI, 0.783-0.950; P<0.001) for AMP challenge, and 0.588 (95% CI, 0.467-0.709, P=0.156) for eNO measurement. The cutoff values of these tests were methacholine PC20 (provocative concentration of methacholine causing a 20% fall in forced expiratory volume in one second) 12.0 mg/mL (sensitivity, 87.9%; specificity, 82.8%), AMP PC20 566.2 mg/mL (sensitivity, 84.8%; specificity, 85.9%), and eNO 18.5 ppb (sensitivity, 45.5%; specificity, 71.9%).
Figures and Tables
 | Fig. 1Recruitment and follow-up of study subjects. PFT, pulmonary function test; Mch, methacholine; AMP, adenosine 5'-monophosphate; eNO, exhaled nitric oxide; SPT, skin prick test. *Bronchopulmonary dysplasia, bronchiolitis obliterans, congenital heart disease.
|
 | Fig. 2Receiver operation characteristic curve for methacholine PC20. PC20, provocative concentration causing a 20% fall in the forced expiratory volume in one second decrease; AUC, area under curve; CI, confidence interval.
|
 | Fig. 3Receiver operation characteristic curve for AMP PC20. AMP, adenosine-5'-monophosphate; PC20, provocative concentration causing a 20% fall in the forced expiratory volume in one second decrease; AUC, area under curve; CI, confidence interval.
|
 | Fig. 4Receiver operation characteristic curve for exhaled nitric oxide. AUC, area under curve; CI, confidence interval.
|
Table 1
Baseline characteristics of study subjects

![]()
Table 2
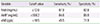
Lung function, bronchial hyperresponsiveness, and exhaled nitric oxide between asthmatic and nonasthmatic children
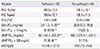
Values are presented as mean±standard deviation (SD), geometric mean (range of 1SD), or number (%).
FEV1, forced expiratory volume in one second; %pred, percentage predicted; FVC, forced vital capacity; Mch, methacholine; PC20, provocative concentration causing a 20% fall in the FEV1; AMP, adenosine-5'-monophosphate; eNO, exhaled nitric oxide.
**P<0.001, compared to nonasthma group.
![]()
References
1. Avital A, Godfrey S, Springer C. Exercise, methacholine, and adenosine 5'-monophosphate challenges in children with asthma: relation to severity of the disease. Pediatr Pulmonol. 2000; 30:207–214.

2. Beckert L, Jones K. Bronchial challenge testing. In : Sapey E, editor. Bronchial asthma - emerging therapeutic strategies. Rijeka (CRO): InTech;2012. p. 19–36.
3. De Meer G, Heederik D, Postma DS. Bronchial responsiveness to adenosine 5'-monophosphate (AMP) and methacholine differ in their relationship with airway allergy and baseline FEV(1). Am J Respir Crit Care Med. 2002; 165:327–331.
4. van den Berge M, Kerstjens HA, Meijer RJ, de Reus DM, Koeter GH, Kauffman HF, et al. Corticosteroid-induced improvement in the PC20 of adenosine monophosphate is more closely associated with reduction in airway inflammation than improvement in the PC20 of methacholine. Am J Respir Crit Care Med. 2001; 164:1127–1132.
5. Van Den Berge M, Meijer RJ, Kerstjens HA, de Reus DM, Koëter GH, Kauffman HF, et al. PC(20) adenosine 5'-monophosphate is more closely associated with airway inflammation in asthma than PC(20) methacholine. Am J Respir Crit Care Med. 2001; 163:1546–1550.
6. Shim E, Lee E, Yang SI, Jung YH, Park GM, Kim HY, et al. The association of lung function, bronchial hyperresponsiveness, and exhaled nitric oxide differs between atopic and non-atopic asthma in children. Allergy Asthma Immunol Res. 2015; 7:339–345.
7. Pijnenburg MW, De Jongste JC. Exhaled nitric oxide in childhood asthma: a review. Clin Exp Allergy. 2008; 38:246–259.
8. Strunk RC, Szefler SJ, Phillips BR, Zeiger RS, Chinchilli VM, Larsen G, et al. Relationship of exhaled nitric oxide to clinical and inflammatory markers of persistent asthma in children. J Allergy Clin Immunol. 2003; 112:883–892.
9. Berkman N, Avital A, Breuer R, Bardach E, Springer C, Godfrey S. Exhaled nitric oxide in the diagnosis of asthma: comparison with bronchial provocation tests. Thorax. 2005; 60:383–388.
10. Dweik RA, Boggs PB, Erzurum SC, Irvin CG, Leigh MW, Lundberg JO, et al. An official ATS clinical practice guideline: interpretation of exhaled nitric oxide levels (FENO) for clinical applications. Am J Respir Crit Care Med. 2011; 184:602–615.
11. Sivan Y, Gadish T, Fireman E, Soferman R. The use of exhaled nitric oxide in the diagnosis of asthma in school children. J Pediatr. 2009; 155:211–216.
12. Ferrante G, Malizia V, Antona R, Corsello G, La Grutta S. The value of FeNO measurement in childhood asthma: uncertainties and perspectives. Multidiscip Respir Med. 2013; 8:50.
13. Kim SH, Yoon HJ. Use of the exhaled nitric oxide for management of asthma and respiratory diseases. Korean J Med. 2008; 74:579–586.
14. National Heart, Lung, and Blood Institute, National Asthma Education and Prevention Program. Expert panel report 3: guidelines for the diagnosis and management of asthma. Full report 2007. NIH publication no. 07-4051 [Internet]. Bethesda (MD): National Heart, Lung, and Blood Institute;2007. cited 2015 Aug 9. Available from: http://www.nhlbi.nih.gov/guidelines/asthma/asthgdln.pdf.
15. Quanjer PH, Stanojevic S, Cole TJ, Baur X, Hall GL, Culver BH, et al. Multi-ethnic reference values for spirometry for the 3-95-yr age range: the global lung function 2012 equations. Eur Respir J. 2012; 40:1324–1343.
16. Crapo RO, Casaburi R, Coates AL, Enright PL, Hankinson JL, Irvin CG, et al. Guidelines for methacholine and exercise challenge testing-1999. This official statement of the American Thoracic Society was adopted by the ATS Board of Directors, July 1999. Am J Respir Crit Care Med. 2000; 161:309–329.
17. Joos GF, O'Connor B, Anderson SD, Chung F, Cockcroft DW, Dahlén B, et al. Indirect airway challenges. Eur Respir J. 2003; 21:1050–1068.
18. Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A, et al. Standardisation of spirometry. Eur Respir J. 2005; 26:319–338.
19. Heinzerling L, Frew AJ, Bindslev-Jensen C, Bonini S, Bousquet J, Bresciani M, et al. Standard skin prick testing and sensitization to inhalant allergens across Europe: a survey from the GALEN network. Allergy. 2005; 60:1287–1300.
20. Brown WG, Halonen MJ, Kaltenborn WT, Barbee RA. The relationship of respiratory allergy, skin test reactivity, and serum IgE in a community population sample. J Allergy Clin Immunol. 1979; 63:328–335.
21. Jang WN, Park IS, Choi CH, Bauer S, Harmin S, Seo SC, et al. Relationships between exhaled nitric oxide and atopy profiles in children with asthma. Allergy Asthma Immunol Res. 2013; 5:155–161.
22. Kovesi T, Kulka R, Dales R. Exhaled nitric oxide concentration is affected by age, height, and race in healthy 9- to 12-year-old children. Chest. 2008; 133:169–175.
23. Henriksen AH, Lingaas-Holmen T, Sue-Chu M, Bjermer L. Combined use of exhaled nitric oxide and airway hyperresponsiveness in characterizing asthma in a large population survey. Eur Respir J. 2000; 15:849–855.
24. Hahn YS. Measurements of fractional exhaled nitric oxide in pediatric asthma. Korean J Pediatr. 2013; 56:424–430.
25. Carlsten C, Dimich-Ward H, Ferguson A, Becker A, Dybuncio A, Chan-Yeung M. Airway hyperresponsiveness to methacholine in 7-year-old children: sensitivity and specificity for pediatric allergist-diagnosed asthma. Pediatr Pulmonol. 2011; 46:175–178.
26. Liem JJ, Kozyrskyj AL, Cockroft DW, Becker AB. Diagnosing asthma in children: what is the role for methacholine bronchoprovocation testing. Pediatr Pulmonol. 2008; 43:481–489.
27. Arga M, Bakirtas A, Topal E, Turktas I. Can exhaled nitric oxide be a surrogate marker of bronchial hyperresponsiveness to adenosine 5'-monophosphate in steroid-naive asthmatic children? Clin Exp Allergy. 2015; 45:758–766.
28. Suh DI, Lee JK, Kim CK, Koh YY. Bronchial hyperresponsiveness to methacholine and adenosine 5'-monophosphate, and the presence and degree of atopy in young children with asthma. Clin Exp Allergy. 2011; 41:338–345.
 XML Download
XML Download