

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Sung-Shin Kwon*, Min-Hye Kim*, Young-Joo Cho
Abstract
Purpose
Asthma is a global health concern involving 300 million people, and mortality due to asthma still accounts for a significant proportion of deaths. The purpose of this study was to define risk factors for the mortality of patients admitted to the intensive care unit because of asthma exacerbation.
Methods
A retrospective analysis of 163 severe asthma patients, who were admitted to Ewha Womans University Mokdong Hospital from January 1997 to December 2011 with the need for intensive medical care, was performed. The medical history and laboratory workup at initial visit to hospital were collected by reviewing medical records. To identify risk factors for mortality, data was compared between the survivors (survivor group) and the dead (death group).
Results
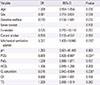
As a result, mortality rate was 30.7%. The number of patients 65 years or older was larger in the death group. The number of patients on mechanical ventilation was larger in the death group compared to the survivor group. In arterial blood gas analysis, the levels of pH and PaO2 were higher and the PCO2 levels were lower in the death group. In multivariate analysis, the risk of death was higher in patients on mechanical ventilation (odds ratio [OR], 5.327). PCO2 and O2 saturation were protective factors for mortality (OR, 0.90 and 0.915, respectively).
Figures and Tables
Table 1
Demographic characteristics of study subjects

![]()
Table 2
Cause of death of severe asthma patient in hospital
| Cause of death | No. of patients (%) |
|---|---|
| Asthma | 18 (36.0) |
| Infection | 25 (50.0) |
| Cardiologic disease | 7 (14.0) |
![]()
Table 3
Comparison of asthma and its treatment history before admission

![]()
Table 4
Clinical characteristics during hospital course

![]()
Table 5
Comparison of initial laboratory finding on admission

![]()
Table 6
Multivariate logistic regression analysis for survival
![]()
References
1. Eder W, Ege MJ, von Mutius E. The asthma epidemic. N Engl J Med. 2006; 355:2226–2235.

2. Lee SI. Prevalence of childhood asthma in Korea: international study of asthma and allergies in childhood. Allergy Asthma Immunol Res. 2010; 2:61–64.
3. Cho SH, Kim YK, Chang YS, Kim SS, Min KU, Kim YY. Asthma insights and reality in Korea. Korean J Med. 2006; 70:69–77.
4. Park HS, Choi GS, Cho JS, Kim YY. Epidemiology and current status of allergic rhinitis, asthma, and associated allergic diseases in Korea: ARIA Asia-Pacific workshop report. Asian Pac J Allergy Immunol. 2009; 27:167–171.
5. Kroegel C. Global initiative for asthma management and prevention-GINA 2006. Pneumologie. 2007; 61:295–304.
6. de Marco R, Locatelli F, Cazzoletti L, Bugianio M, Carosso A, Marinoni A. Incidence of asthma and mortality in a cohort of young adults: a 7-year prospective study. Respir Res. 2005; 6:95.
7. Dantzer C, Tessier JF, Nejjari C, Barberger-Gateau P, Dartigues JF. Mortality of elderly subjects with self-reported asthma in a French cohort, 1991-1996. Eur J Epidemiol. 2001; 17:57–63.
8. Huovinen E, Kaprio J, Vesterinen E, Koskenvuo M. Mortality of adults with asthma: a prospective cohort study. Thorax. 1997; 52:49–54.
9. Pendergraft TB, Stanford RH, Beasley R, Stempel DA, Roberts C, McLaughlin T. Rates and characteristics of intensive care unit admissions and intubations among asthma-related hospitalizations. Ann Allergy Asthma Immunol. 2004; 93:29–35.
10. Campbell MJ, Cogman GR, Holgate ST, Johnston SL. Age specific trends in asthma mortality in England and Wales, 1983-95: results of an observational study. BMJ. 1997; 314:1439–1441.
11. Hansell A, Hollowell J, McNiece R, Nichols T, Strachan D. Validity and interpretation of mortality, health service and survey data on COPD and asthma in England. Eur Respir J. 2003; 21:279–286.
12. Cho SH, Park HW, Rosenberg DM. The current status of asthma in Korea. J Korean Med Sci. 2006; 21:181–187.
13. Kim MS, Cho YJ, Moon HB, Cho SH. Factors for poor prognosis of near-fatal asthma after recovery from a life-threatening asthma attack. Korean J Intern Med. 2008; 23:170–175.
14. Rodrigo GJ, Plaza V, Forns SB, Tordera MP, Salas J. Factors associated with mortality in patients hospitalized in Spain and Latin America for acute severe asthma in 1994, 1999, and 2004. J Bras Pneumol. 2008; 34:546–551.
15. Park JH, Moon HB, Na JO, Song HH, Lim CM, Lee MS, et al. The predictable factors for the mortality of fatal asthma with acute respiratory failure. Tuberc Respir Dis. 1999; 47:356–364.
16. Ringbaek T, Seersholm N, Viskum K. Standardised mortality rates in females and males with COPD and asthma. Eur Respir J. 2005; 25:891–895.
17. Tan WC, Xiang X, Qiu D, Ng TP, Lam SF, Hegele RG. Epidemiology of respiratory viruses in patients hospitalized with near-fatal asthma, acute exacerbations of asthma, or chronic obstructive pulmonary disease. Am J Med. 2003; 115:272–277.
18. Sturdy PM, Butland BK, Anderson HR, Ayres JG, Bland JM, Harrison BD, et al. Deaths certified as asthma and use of medical services: a national case-control study. Thorax. 2005; 60:909–915.
 XML Download
XML Download