

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Sung Do Moon1, 2, Ha Kyung Won1, 2, Jae-Young Cho1, Min-Koo Kang1, 2, Ju-Young Kim1, 2, 3, Han-Ki Park1, 2, 3, Sujeong Kim4, Hye-Ryun Kang1, 2, 3
Abstract
For the treatment of multidrug-resistant (MDR) tuberculosis, maintenance of appropriate antituberculous agents is essential because of its low cure rate and high dropout rate. Drug reaction with eosinophilia and systemic symptoms (DRESS) syndrome is a severe drug-induced systemic hypersensitivity response resulting in cessation of causative agents. In cases of second-line antituberculous agent-induced DRESS, it is extremely difficult to find other replacement medications to cure MDR tuberculosis. A 53-year-old male who had taken the second-line antituberculous agents (cycloserine, streptomycin, p-aminosalicylic acid, and prothionamide) as well as pyrazinamide for 5 weeks experienced DRESS syndrome accompanying hepatic coma. His symptoms improved with discontinuation of antituberculous agents and administration of high-dose methylprednisolone for 1 month. To resume the antituberculous medication, second-line antituberculous agents were administered one by one using a rapid desensitization protocol. While kanamycin, levofloxacin, and cycloserine were successfully readministered, p-aminosalicylic acid- and prothionamide-induced cutaneous hypersensitivity symptoms were relatively mild compared to previous reactions. Herein, we report a case of successfully treated MDR tuberculosis having a history of fatal DRESS syndrome to antituberculous agents using the rapid desensitization protocol.
Figures and Tables
 | Fig. 1Skin findings of patch test to antitubercular drugs read at 48 hours. Test drugs are isoniazid (INH), levofloxacin (LV), prothinamide (PTH), p-aminosalicylic acid (PAS), streptomycin (SM), ethambutol (ETM), cycloserine (CS), amoxicillin clavulanate (Am), pyrazinamide (Pyz), rifampicin (RFP) in clockwise direction from the right top.
|
Table 1
Summary of drug administration and related symptoms

● , administration of full dose; □ , discontinuation; ▲ , administration with desensitization protocol; △ , hypersensitivity reaction despite administration with desensitization protocol; PZA, pyrazinamide; SM, streptomycin; CS, cycloserine; PAS, p-aminosalicylic acid; PTH, prothionamide; LVFX, levofloxacin; KM, kanamycin; AC, amoxicillin clavulanate.
![]()
Table 2
Intravenous rapid desensitization protocol for kanamycin (target dose: 1,000 mg)
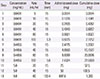
![]()
Table 3
Oral rapid desensitization protocol for prothionamide (target dose: 250 mg twice a day)
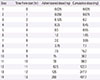
![]()
Table 4
Oral rapid desensitization protocol for cycloserine (target dose: 500 mg twice a day)
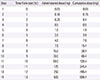
![]()
References
1. World Health Organization. Global tuberculosis report 2013 [Internet]. Geneva: World Health Organization;2013. cited 2014 Apr 1. www.who.int/iris/bitstream/10665/91355/1/9789241564656_eng.pdf.
2. Kim HJ. Current status of tuberculosis in Korea. Korean J Med. 2012; 82:257–262.

3. Kim DH, Kim HJ, Park SK, Kong SJ, Kim YS, Kim TH, et al. Treatment outcomes and long-term survival in patients with extensively drug-resistant tuberculosis. Am J Respir Crit Care Med. 2008; 178:1075–1082.
4. Walsh SA, Creamer D. Drug reaction with eosinophilia and systemic symptoms (DRESS): a clinical update and review of current thinking. Clin Exp Dermatol. 2011; 36:6–11.
5. Cacoub P, Musette P, Descamps V, Meyer O, Speirs C, Finzi L, et al. The DRESS syndrome: a literature review. Am J Med. 2011; 124:588–597.
6. Galvao VR, Aun MV, Kalil J, Castells M, Giavina-Bianchi P. Clinical and laboratory improvement after intravenous immunoglobulin in drug reaction with eosinophilia and systemic symptoms. J Allergy Clin Immunol Pract. 2014; 2:107–110.
7. Joly P, Janela B, Tetart F, Rogez S, Picard D, D'Incan M, et al. Poor benefit/risk balance of intravenous immunoglobulins in DRESS. Arch Dermatol. 2012; 148:543–544.
8. Santhamoorthy P, Alexander KJ, Alshubaili A. Intravenous immunoglobulin in the treatment of drug rash eosinophilia and systemic symptoms caused by phenytoin. Ann Indian Acad Neurol. 2012; 15:320–322.
9. Chiriac AM, Demoly P. Multiple drug hypersensitivity syndrome. Curr Opin Allergy Clin Immunol. 2013; 13:323–329.
10. Scherer K, Brockow K, Aberer W, Gooi JH, Demoly P, Romano A, et al. Desensitization in delayed drug hypersensitivity reactions: an EAACI position paper of the Drug Allergy Interest Group. Allergy. 2013; 68:844–852.
11. Holland CL, Malasky C, Ogunkoya A, Bielory L. Rapid oral desensitization to isoniazid and rifampin. Chest. 1990; 98:1518–1519.
12. Matz J, Borish LC, Routes JM, Rosenwasser LJ. Oral desensitization to rifampin and ethambutol in mycobacterial disease. Am J Respir Crit Care Med. 1994; 149(3 Pt 1):815–817.
 XML Download
XML Download