

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Min Ah Cha, Yeol Ryoon Woo, Hyun Jin Kim, Min Sub Kim, Yeon Hwa Ahn
Abstract
Purpose
Both under-nutrition and obesity may be associated with severity of viral infection. We investigated the association of obesity with clinical factors and the severity of acute bronchiolitis in infants.
Methods
We reviewed 740 infants younger than 1 year of age who were admitted with the first episode of acute bronchiolitis between 2010 and 2013. Subjects were classified into 3 groups according to the weight-for-length Z-score.
Results
Younger age (3.6±2.6 months) was more frequent in the obesity group (P<0.001). Infants aged ≤6 months (90%) dominantly included in the obesity group. Logistic regression showed that age (younger than 3 months) was independently associated with the overweight and obesity groups with acute bronchiolitis in infants (odds ratio [OR], 1.77; P=0.001 for overweight; OR, 4.67; P<0.001 for obesity). Moreover, the obesity group was associated with an increased risk of chest retraction, hypoxia, respiratory syncytial virus detection, length of stay (more than 5 days), and need for oxygen supplement. These factors tended to increase from the overweight group toward the obesity group.
Figures and Tables
Fig. 1
Age distribution in normal, overweight, and obesity groups with acute bronchiolitis in infants.

Table 1
Dermographic and clinical characteristics of the subjects (n=740)

Values are presented as mean±standard deviation or number (%).
WFL, weight-for-length; RSV, respiratory syncytial virus.
*Normal, -2≤WFL Z-score<1; overweight, 1≤WFL Z-score<3; obesity, 3≤WFL Z-score. †1-3 months, respiratory rate≥55/min; 4-6 months, respiratory rate≥50/min; 7-12 months, respiratory rate≥45/min. ‡Percutaneous oxygen saturation<95%. §Fever episode in total duration of disease. ∥Supplement oxygen when percutaneous oxygen saturation<95%.
Table 2
Comparison of clinical factor between normal, overweight, and obesity groups
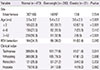
Table 3
Comparison of severity between normal, overweight, and obesity groups

Table 4
Risk factors in overweight and obesity group with acute bronchiolitis in infants*

References
1. Bueno FU, Piva JP, Garcia PC, Lago PM, Einloft PR. Outcome and characteristics of infants with acute viral bronchiolitis submitted to mechanical ventilation in a Brazilian pediatric intensive care. Rev Bras Ter Intensiva. 2009; 21:174–182.

2. Simoes EA. Environmental and demographic risk factors for respiratory syncytial virus lower respiratory tract disease. J Pediatr. 2003; 143:5 Suppl. S118–S126.
3. Kim HJ, Kim JH, Kang IJ. Association of respiratory viral infection and atopy with severity of acute bronchiolitis in infants. Pediatr Allergy Respir Dis. 2011; 21:302–312.
4. Morgan OW, Bramley A, Fowlkes A, Freedman DS, Taylor TH, Gargiullo P, et al. Morbid obesity as a risk factor for hospitalization and death due to 2009 pandemic influenza A(H1N1) disease. PLoS One. 2010; 5:e9694.
5. Akiyama N, Segawa T, Ida H, Mezawa H, Noya M, Tamez S, et al. Bimodal effects of obesity ratio on disease duration of respiratory syncytial virus infection in children. Allergol Int. 2011; 60:305–308.
6. Tracey VV, De NC, Harper JR. Obesity and respiratory infection in infants and young children. Br Med J. 1971; 1:16–18.
7. Shibli R, Rubin L, Akons H, Shaoul R. Morbidity of overweight (>or=85th percentile) in the first 2 years of life. Pediatrics. 2008; 122:267–272.
8. Jedrychowski W, Maugeri U, Flak E, Mroz E, Bianchi I. Predisposition to acute respiratory infections among overweight preadolescent children: an epidemiologic study in Poland. Public Health. 1998; 112:189–195.
9. Rivera Claros R, Marin V, Castillo-Duran C, Jara L, Guardia S, Díaz N. Nutritional status and clinical evolution of hospitalized Chilean infants with infection by respiratory syncytial virus (RSV). Arch Latinoam Nutr. 1999; 49:326–332.
10. Jung HJ, Kim MJ, Lee K, Kim HJ, Byun SO. Factors influencing recurrent wheezing in infants: the relationship between respiratory syncytial virus infections and the development of recurrent wheezing. Pediatr Allergy Respir Dis. 2011; 21:319–325.
11. Cole TJ, Bellizzi MC, Flegal KM, Dietz WH. Establishing a standard definition for child overweight and obesity worldwide: international survey. BMJ. 2000; 320:1240–1243.
12. Moon JS, Lee SY, Nam CM, Choi JM, Choe BK, Seo JW, et al. 2007 Korean National Growth Charts: review of developmental process and an outlook. Korean J Pediatr. 2008; 51:1–25.
13. Garcia CG, Bhore R, Soriano-Fallas A, Trost M, Chason R, Ramilo O, et al. Risk factors in children hospitalized with RSV bronchiolitis versus non-RSV bronchiolitis. Pediatrics. 2010; 126:e1453–e1460.
14. Saunders M, Gorelick MH. Evaluation of the sick child in the office and clinic. In : Kliegman RM, Stanton BF, St. Geme JW, Schor NF, Behrman RE, editors. Nelson textbook of pediatrics. 19th ed. Philadelphia: Elsevier/Saunders;2011. p. 280.
15. Kim KH, Hwang J, Song JH, Lee YS, Kwon JW, Suh DI, et al. Association between the clinical index and disease severity in infants with acute bronchiolitis. Allergy Asthma Respir Dis. 2013; 1:377–382.
16. Damore D, Mansbach JM, Clark S, Ramundo M, Camargo CA Jr. Prospective multicenter bronchiolitis study: predicting intensive care unit admissions. Acad Emerg Med. 2008; 15:887–894.
17. Stensballe LG, Kristensen K, Simoes EA, Jensen H, Nielsen J, Benn CS, et al. Atopic disposition, wheezing, and subsequent respiratory syncytial virus hospitalization in Danish children younger than 18 months: a nested case-control study. Pediatrics. 2006; 118:e1360–e1368.
18. Adair LS. Child and adolescent obesity: epidemiology and developmental perspectives. Physiol Behav. 2008; 94:8–16.
19. Victora CG, Morris SS, Barros FC, de Onis M, Yip R. The NCHS reference and the growth of breast- and bottle-fed infants. J Nutr. 1998; 128:1134–1138.
20. Kramer MS, Guo T, Platt RW, Shapiro S, Collet JP, Chalmers B, et al. Breastfeeding and infant growth: biology or bias? Pediatrics. 2002; 110(2 Pt 1):343–347.
21. Tal A, Bavilski C, Yohai D, Bearman JE, Gorodischer R, Moses SW. Dexamethasone and salbutamol in the treatment of acute wheezing in infants. Pediatrics. 1983; 71:13–18.
22. Baumer JH. SIGN guideline on bronchiolitis in infants. Arch Dis Child Educ Pract Ed. 2007; 92:ep149–ep151.
23. Shaw KN, Bell LM, Sherman NH. Outpatient assessment of infants with bronchiolitis. Am J Dis Child. 1991; 145:151–155.
24. Plint AC, Johnson DW, Wiebe N, Bulloch B, Pusic M, Joubert G, et al. Practice variation among pediatric emergency departments in the treatment of bronchiolitis. Acad Emerg Med. 2004; 11:353–360.
25. Jee HM, Seo HK, Hyun SE, Yoo EG, Kim CH, Han MY. Association of higher adiposity and wheezing in infants with lower respiratory illnesses. Acta Paediatr. 2010; 99:1365–1369.
26. Wang EE, Milner RA, Navas L, Maj H. Observer agreement for respiratory signs and oximetry in infants hospitalized with lower respiratory infections. Am Rev Respir Dis. 1992; 145:106–109.
27. Wainwright C. Acute viral bronchiolitis in children: a very common condition with few therapeutic options. Paediatr Respir Rev. 2010; 11:39–45.
28. El-Radhi AS, Barry W, Patel S. Association of fever and severe clinical course in bronchiolitis. Arch Dis Child. 1999; 81:231–234.
29. Marguet C, Lubrano M, Gueudin M, Le Roux P, Deschildre A, Forget C, et al. In very young infants severity of acute bronchiolitis depends on carried viruses. PLoS One. 2009; 4:e4596.
 XML Download
XML Download