

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
Although methacholine PC20 helps clinicians to identify asthma, there are practical limitations in using methacholine PC20 to assess asthma control. We assessed the relationship between methacholine PC20 levels and asthma control status in child patients with atopic asthma.
Methods
We enrolled 153 children of 8 to 15 years of age with atopic asthma and measured methacholine PC20 of these children when their asthma was controlled. We followed up these patients for more than 2 years with measurements of asthma control score, lung function, bronchodilator response (BDR), and fractional exhaled nitric oxide (FeNO).
Results
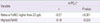
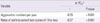
The geometric mean of methacholine PC20 in the study population was 2.81 mg/mL. Lower methacholine PC20 was found to be associated with lower lung function, higher rate of BDR greater than 12%, higher level of BDR, higher rate of FeNO levels greater than 23 ppb, higher FeNO, higher numbers of asthma aggravation per year, and higher rate of asthma control test scores of 19 or less.
Figures and Tables
 | Fig. 1Study schedule. PC20, provocative concentration causing 20% fall in forced expiratory volume in 1 second; FeNO, fraction of exhaled nitric oxide.
|


References
1. Busse WW. The relationship of airway hyperresponsiveness and airway inflammation: airway hyperresponsiveness in asthma: its measurement and clinical significance. Chest. 2010. 138:2 Suppl. 4S–10S.
2. Cockcroft DW, Davis BE. Mechanisms of airway hyperresponsiveness. J Allergy Clin Immunol. 2006. 118:551–559.

3. O'Byrne PM, Gauvreau GM, Brannan JD. Provoked models of asthma: what have we learnt? Clin Exp Allergy. 2009. 39:181–192.
4. Sumino K, Sugar EA, Irvin CG, Kaminsky DA, Shade D, Wei CY, et al. Methacholine challenge test: diagnostic characteristics in asthmatic patients receiving controller medications. J Allergy Clin Immunol. 2012. 130:69–75.e6.
5. Cockcroft D, Davis B. Direct and indirect challenges in the clinical assessment of asthma. Ann Allergy Asthma Immunol. 2009. 103:363–369.
6. Sont JK, Han J, van Krieken JM, Evertse CE, Hooijer R, Willems LN, et al. Relationship between the inflammatory infiltrate in bronchial biopsy specimens and clinical severity of asthma in patients treated with inhaled steroids. Thorax. 1996. 51:496–502.
7. Rosi E, Ronchi MC, Grazzini M, Duranti R, Scano G. Sputum analysis, bronchial hyperresponsiveness, and airway function in asthma: results of a factor analysis. J Allergy Clin Immunol. 1999. 103(2 Pt 1):232–237.
8. National Heart, Lung and Blood Institute. National asthma education and prevention program. Expert panel report 3: guidelines for the diagnosis and management of asthma. Full report 2007 [Internet]. cited 2012 Nov 13. Bethesda: National Heart, Lung and Blood Institute;Available from: http://www.nhlbi.nih.gov/guidelines/asthma/asthgdln.pdf.
9. The Global Initiative for Asthma. GINA Report, Global Strategy for Asthma Management and Prevention. Updated Dec. 2011 [Internet]. c2011. cited 2012 Nov 13. The Global Initiative for Asthma;Available from: http://www.ginasthma.org/guidelines-gina-report-global-strategy-for-asthma.html.
10. Nathan RA, Sorkness CA, Kosinski M, Schatz M, Li JT, Marcus P, et al. Development of the asthma control test: a survey for assessing asthma control. J Allergy Clin Immunol. 2004. 113:59–65.
11. Liu AH, Zeiger R, Sorkness C, Mahr T, Ostrom N, Burgess S, et al. Development and cross-sectional validation of the Childhood Asthma Control Test. J Allergy Clin Immunol. 2007. 119:817–825.
12. Hankinson JL, Odencrantz JR, Fedan KB. Spirometric reference values from a sample of the general U.S. population. Am J Respir Crit Care Med. 1999. 159:179–187.
13. Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A, et al. Standardisation of spirometry. Eur Respir J. 2005. 26:319–338.
14. Crapo RO, Casaburi R, Coates AL, Enright PL, Hankinson JL, Irvin CG, et al. Guidelines for methacholine and exercise challenge testing-1999. This official statement of the American Thoracic Society was adopted by the ATS Board of Directors, July 1999. Am J Respir Crit Care Med. 2000. 161:309–329.
15. Recommendations for standardized procedures for the on-line and off-line measurement of exhaled lower respiratory nitric oxide and nasal nitric oxide in adults and children-1999. This official statement of the American Thoracic Society was adopted by the ATS Board of Directors, July 1999. Am J Respir Crit Care Med. 1999. 160:2104–2117.
16. Cockcroft DW. Direct challenge tests: airway hyperresponsiveness in asthma: its measurement and clinical significance. Chest. 2010. 138:2 Suppl. 18S–24S.
17. Weiss ST, Van Natta ML, Zeiger RS. Relationship between increased airway responsiveness and asthma severity in the childhood asthma management program. Am J Respir Crit Care Med. 2000. 162:50–56.
18. Ichinose M, Takahashi T, Sugiura H, Endoh N, Miura M, Mashito Y, et al. Baseline airway hyperresponsiveness and its reversible component: role of airway inflammation and airway calibre. Eur Respir J. 2000. 15:248–253.
19. De Meer G, Heederik D, Postma DS. Bronchial responsiveness to adenosine 5'-monophosphate (AMP) and methacholine differ in their relationship with airway allergy and baseline FEV(1). Am J Respir Crit Care Med. 2002. 165:327–331.
20. Colon-Semidey AJ, Marshik P, Crowley M, Katz R, Kelly HW. Correlation between reversibility of airway obstruction and exhaled nitric oxide levels in children with stable bronchial asthma. Pediatr Pulmonol. 2000. 30:385–392.
21. Synek M, Beasley R, Frew AJ, Goulding D, Holloway L, Lampe FC, et al. Cellular infiltration of the airways in asthma of varying severity. Am J Respir Crit Care Med. 1996. 154:224–230.
22. Szefler SJ, Leung DY. Severe asthma: pathogenesis and clinical management. 1996. New York: Marcel Dekker.
23. Suh DI, Lee JK, Lee JH, Koh YY. Bronchodilator response and its relationship to bronchial hyperresponsiveness in children with allergic rhinitis/asthma. Pediatr Allergy Respir Dis. 2010. 20:59–67.
24. Short PM, Lipworth SI, Lipworth BJ. Relationships between airway hyperresponsiveness, inflammation, and calibre in asthma. Lung. 2011. 189:493–497.
25. Langley SJ, Goldthorpe S, Custovic A, Woodcock A. Relationship among pulmonary function, bronchial reactivity, and exhaled nitric oxide in a large group of asthmatic patients. Ann Allergy Asthma Immunol. 2003. 91:398–404.
26. Crimi E, Spanevello A, Neri M, Ind PW, Rossi GA, Brusasco V. Dissociation between airway inflammation and airway hyperresponsiveness in allergic asthma. Am J Respir Crit Care Med. 1998. 157:4–9.
27. Reid DW, Johns DP, Feltis B, Ward C, Walters EH. Exhaled nitric oxide continues to reflect airway hyperresponsiveness and disease activity in inhaled corticosteroid-treated adult asthmatic patients. Respirology. 2003. 8:479–486.
28. Berlyne GS, Parameswaran K, Kamada D, Efthimiadis A, Hargreave FE. A comparison of exhaled nitric oxide and induced sputum as markers of airway inflammation. J Allergy Clin Immunol. 2000. 106:638–644.
29. Brightling CE, Symon FA, Birring SS, Bradding P, Wardlaw AJ, Pavord ID. Comparison of airway immunopathology of eosinophilic bronchitis and asthma. Thorax. 2003. 58:528–532.
30. Warke TJ, Fitch PS, Brown V, Taylor R, Lyons JD, Ennis M, et al. Exhaled nitric oxide correlates with airway eosinophils in childhood asthma. Thorax. 2002. 57:383–387.
31. Woo SI, Lee JH, Kim H, Kang JW, Sun YH, Hahn YS. Utility of fractional exhaled nitric oxide (F(E)NO) measurements in diagnosing asthma. Respir Med. 2012. 106:1103–1109.
 XML Download
XML Download