

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Cutaneous adverse drug reactions account for about 30% of all adverse drug reactions and are observed in 2-3% of hospitalized patients.1-3) Severe cutaneous drug reactions include Stevens-Johnson syndrome, toxic epidermal necrolysis, acute generalized exanthematous pustulosis, and drug rash with eosinophilia and systemic symptoms syndrome (DRESS syndrome).4,5) The diagnosis of DRESS syndrome, named drug-induced pseudolymphoma or drug hypersensitivity syndrome in the past, proposed by Bocquet et al.6), is based on the following three criteria: 1) cutaneous drug eruption; 2) hematologic abnormalities, including eosinophilia (>1.5×109 eosinophils/L) or the presence of atypical lymphocytes; and 3) systemic involvement, including adenopathies >2 cm in diameter, hepatitis (transaminase values >2 times normal), interstitial nephritis, interstitial pneumonia, or carditis. Histological evaluation of lymph nodes of the patients with DRESS syndrome often shows a lymphoma-like pattern and DRESS syndrome has been confused with malignant lymphoma.7,8) Cases in which DRESS syndrome presents with lymphoma are associated with a lower probability of malignancy, which is associated with atypical lymphocytes and necessitates consideration of skin or lymph node biopsies.7,8) We report here a case of T-cell lymphoma which presented as DRESS syndrome caused by non-steroidal anti-inflammatory drug (NSAID).
CASE REPORT
On July 3, 2012, a 41-year-old female patient visited our dermatology department for evaluation of an erythematous skin lesion with itching on her abdomen and both thighs. She had no history of allergy, including drug or food allergy. Moreover, she had no medical history. Erythematous pruritic plaques were scattered on both thighs and lasted for several days. The assessment of dermatologists was urticarial dermatitis, and an antihistamine with systemic steroid (prednisolone 30 mg per day) was prescribed. During the following 1 month, her skin lesion improved until she started taking additional medication, including naproxen, due to myalgia that developed after she climbed a mountain. She stopped taking naproxen 3 days later because her skin rash worsened. After 2 days not taking the drugs, her myalgia recurred and she took another medication containing dexibuprofen. One day later, she visited an emergency department because the skin rash had spread over her whole body and she had facial edema (Fig. 1). The initial assessment was that she was suffering from drug eruption caused by NSAIDs.
On admission, her vital signs were a blood pressure of 100/60 mmHg, a heart rate of 96 beats/min, a respiratory rate of 14 breaths/min, and a body temperature of 39.1℃. Confluent erythematous swollen maculopapaules over her whole body and lymphadenopathies in cervical and inguinal areas were found upon physical examination. All of the lymph nodes were nontender, firm, and sized less than 1 cm in diameter. Laboratory test results were as follows: hemoglobin (Hb), 9.5 g/dL; white blood cells, 10,900/mm3 (segmented neutrophils, 66.9%; lymphocytes, 22.2%; and eosinophils, 0.6%); platelets, 208,000/mm3; total bilirubin, 1.4 mg/dL; aspartate aminotransferase/alanine aminotransferase (AST/ALT), 81/137 U/L; lactate dehydrogenase, 694 U/L (normal range, 100 to 200 U/L); and prothrombin time/activated partial thromboplastin time, 12.5/26 seconds. The patient showed negative results for hepatitis B surface antigen, antihepatitis C virus antibody (Ab), and antihuman immunodeficiency Ab, and a positive result for hepatitis B surface antibody. Also, she showed a negative result for antinuclear Ab and rheumatoid factor. Serologic tests for Epstein-Barr virus, cytomegalovirus, herpes simplex virus, and varicella zoster virus infections were all negative and there was no evidence of bacterial growth. The β2-microglobulin level was 6.5 mg/dL (normal range, 0.8 to 2.2 mg/dL).
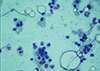
After initial assessment of the drug-associated eruption, the patient was treated with systemic steroid (dexamethasone, 10 mg per day). Her clinical symptoms improved initially, however, even although several days' treatment, her fever remained and her skin lesions became progressively aggravated. Further laboratory tests gave the following results: Hb, 8.3 g/dL; white blood cells, 23,100/mm3 (segmented neutrophils, 24.6%; lymphocytes, 60.5%; and eosinophils, 0.2%), platelets, 106,000/mm3; total bilirubin, 3.0 mg/dL; and AST/ALT, 392/444 U/L. Moreover, atypical lymphocytes were observed in a peripheral blood smear. The patient was transferred to the department of allergy and clinical immunology with a diagnosis of DRESS syndrome, based on clinical features of cutaneous drug eruptions, presence of atypical lymphocytes, and hepatitis after taking NSAID. Using scoring system for classifying DRESS cases (RegiSCAR scoring system)9), the patient scored at least score 5, which contained enlarged lymph node, atypical lymphocytes, skin rash extent (% body surface area) >50%, organ involvement (liver), and none of other potential causes, indicating "probable case". Because the patient could not stop the current medications, a patch test to naproxen was not available. After her admittance, she was treated with high dose systemic steroid (methylprednisolone, 125 mg) and intravenous immunoglobulin (0.4 mg/kg). Although after 2 days of these treatments, her fever persisted and laboratory parameters were aggravated: Hb, 7.2 g/dL; white blood cells, 21,000/mm3 (segmented neutrophils, 18.0%; lymphocytes, 68.0%; and atypical lymphocytes, 6.0%); platelets, 60,000/mm3; total bilirubin, 2.1 mg/dL; and AST/ALT, 144/327 U/L. A cervical lymph node biopsy showed atypical lymphoid hyperplasia and a skin biopsy of abdomen showed perivascular atypical lymphoid cell infiltration. To rule out underlying lymphoid malignancies, a bone marrow biopsy was performed. The bone marrow biopsy revealed interstitial infiltration by neoplastic cells positive for CD3, CD4, CD5, CD7, CD8, CD38, and human leukocyte antigens-DR (Fig. 2). Her final diagnosis was T-cell lymphoma which presented as DRESS syndrome. After four cycles of chemotherapy, she was treated with allo-peripheral blood stem cell transplantation on December 21, 2012 and was discharged without any sequelae. No evidence of recurrence or skin lesion to date has been noted.
DISCUSSION
Our patient fulfilled the DRESS syndrome diagnostic criteria proposed by Bocquet et al.6): cutaneous drug eruptions, the presence of atypical lymphocytes, and hepatitis. The drugs causative of DRESS syndrome are anticonvulsants (such as carbamazepine, phenytoin, phenobarbital, zonisamide, and lamotrigine), allopurinol, minocycline, dapsone, sulfasalazine, mexiletine hydrochloride, antibiotics, and NSAIDs.10,11) Because our patient had initiated NSAID treatment 2 weeks previously when she was transferred to the department of allergy and clinical immunology, we diagnosed her with DRESS syndrome caused by NSAID. However, after systemic steroid and intravenous immunoglobulin treatment, the condition of the patient did not improve and her hematologic abnormalities worsened. Although atypical lymphocytes are a feature of DRESS syndrome, we conducted a bone marrow biopsy to rule out underlying lymophoproliferative disorders. Surprisingly, the bone marrow biopsy showed malignant peripheral T-cell lymphoma involving the bone marrow. Therefore, her final diagnosis was a peripheral T-cell lymphoma which presented as DRESS syndrome. After proper treatment of lymphoma, her systemic symptoms and all the findings including lymphadenopathy were completely improved.
In this patients, the lymphadenopathy, fever, and atypical lymphocytes in peripheral blood suggested lymphoma. Reactive lymphoid disorders, such as Kikuchi's lymphadenitis, infectious mononucleosis, and autoimmune lymphoproliferative syndrome, are sometimes misdiagnosed as malignant lymphoma, and the opposite also occurs.12) DRESS syndrome includes eosinophilia as a characteristic, while Th2-type immune responses may be involved and T-cell abnormalities may exist.13) Because there is no way to distinguish atypical lymphocytes in DRESS syndrome from atypical lymphocytes in lymphoma, thorough observation of an atypical clinical course and poor response to full doses of anti-inflammatory treatments, such as high-dose systemic steroid and intravenous immunoglobulin therapy, may suggest underlying lymphoproliferative conditions. This case suggested that when diagnosing DRESS syndrome, we should give careful consideration to lymphadenopathy and atypical lymphocytes, which also can be a presentation of lymphoma and mimic pseudolymphoma and lymphoma. Clinicians should carefully observe patient's response to anti-inflammatory treatments after diagnosis with DRESS syndrome.

 XML Download
XML Download