

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Despite recent advances in medicine, no significant improvement has been achieved in therapeutic outcomes for severe traumatic brain injury (TBI). In particular, acute subdural hematoma (ASDH) with multiple traumas has remained a severe brain injury with a high mortality rate.3142526)
In the treatment of severe multiple traumas, accurate judgment and prompt action corresponding to rapid pathophysiological changes are required, but in not a few cases, the best treatment timing for brain damage has unfortunately been missed.5162128)
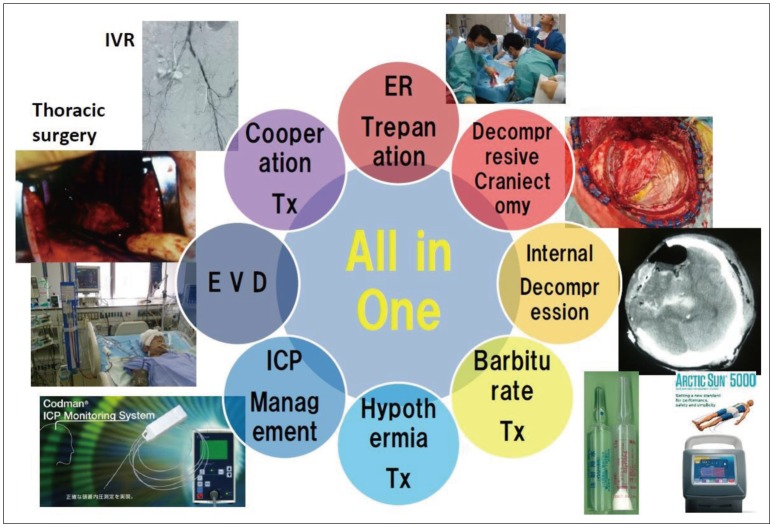
We developed and implemented the “All-in-One” therapeutic strategy consisting of all selectable treatments at the initial stages (Figure 1).
In this study, we report preliminary outcomes of the “All-in-One” therapeutic strategy in severe TBI and discuss the therapeutic efficacy and limitations.
Go to : 
Materials and Methods
This retrospective study examined 158 consecutive patients, who underwent neurosurgical treatments, among 439 patients diagnosed as having traumatic intracranial injuries and then transferred to the High Critical Care and Emergency Center at Nara Medical University Hospital, from April 2007 to December 2015.
All patients were initially treated according to the initial clinical practice guidelines developed by the Japan Advanced Trauma Evaluation and Care (JATEC). Subsequently, for the patients with severe TBI, particularly severe ASDHs, the “All-in-One” therapeutic strategy was adopted to enforce all selectable treatments at the initial stages. The characteristics of our policy are to introduce the following therapy in all cases of Glasgow Coma Scale (GCS) score of ≤8 at the initial treatment stages.
First, in order to rapidly reduce intracranial pressure (ICP), the hematoma is removed by trepanation surgery in the emergency room (ER). In brief, a burr hole is opened performed with a hand drill at the thickest point of the hematoma. In many cases, a small incision in the dura is then made, and the subdural hematoma is ejected from the dural opening. Subsequently, a catheter is placed in the subdural space in order to remove as much hematoma as possible. It is very important to reduce ICP at the earliest for severe TBI patients. We should not wait until the operating room (OR) is available.
Next, if the consciousness level and pupil findings improve, the patient would be transported to an OR. Shortly thereafter, the residual subdural hematoma would be evacuated, and extensive decompression craniotomy (DC) would be performed.
Subsequently, the combined mild hypothermia (deep body temperature, 35℃) and moderate barbiturate (thiamylal sodium, 3-5 mg/kg/h) therapy (H-B therapy) will be performed, and the treatment will continue for 3 to 5 days.202122) Hypothermia management usually with Arctic Sun® 5000 (Medivance Corp, Louisville, Co., USA) is performed on the cooling blanket. In many cases, this combination therapy is initiated during surgery in the OR.
However, if ICP is uncontrollable despite the serial therapeutic management, an internal decompression surgery, including evacuation of traumatic intracerebral hematoma (ICH), would be considered and added as the final treatment option, particularly for pediatric and young patients.7) In principle, internal decompression surgery or removal of cerebral contusion is not conducted as an initial treatment. This is because the preservation of remaining brain function will improve the prognosis of impaired neurological function.
Another treatment option for intractable ICP elevation is external ventricular drainage (EVD) management. This method is recommended as a potential treatment in the new guideline.7) In our treatment strategy, EVD alone as initial therapy has been found to have significant therapeutic limitations; therefore, EVD is only recommended as a complementary treatment option. However, if ICP is uncontrollable, the EVD management would be considered as a treatment option. In fact, EVD management cannot be used alone and is actually implemented in combination with internal decompression surgery or removal of conductional hematoma.
In this study, the results were analyzed statistically using chi-squared test. A p value of less than was considered as statistically significance.
Illustrative case
Case: A 10-year-old girl, traffic accident
This patient was hit by a car while walking and was initially treated in a local hospital. As her abdominal pain gradually worsened, she was transferred to the High Critical Care and Emergency Center. First, a primary survey was performed, and blunt abdominal trauma was diagnosed. When transferred to the center, her GCS score was 14 points, and initial head computed tomography (CT) revealed no obvious intracranial hemorrhage (Figure 2A and B). A hemostasis treatment was administered by a radiologist because of hepatic arterial injury. During transcatheter arterial chemoembolization by the radiation therapy team, the patient's pupils dilated in a short time, and her GCS score deteriorated to 3. After the left subdural hematoma was detected, trepanation surgery was performed in the ER to evacuate as much hematoma as possible, and she was then transferred to the OR immediately.
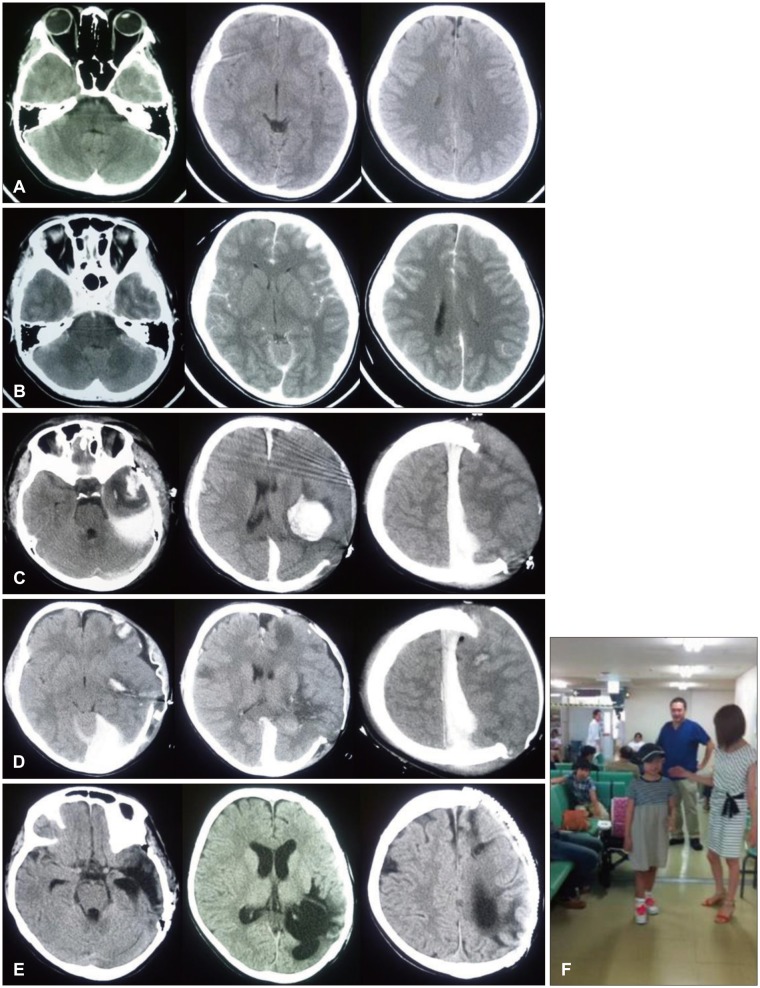 | FIGURE 2(A) Initial computed tomography (CT) showed no obvious intracranial hemorrhage. (B) After transarterial embolization therapy, CT revealed the left subdural hematoma and diminished ambient cistern. (C) CT just after decompressive craniotomy surgery revealed traumatic intracerebral hematoma (ICH) and severe brain bulging. (D) CT after the second surgery showed removal of traumatic ICH and left temporal lobectomy as internal decompression surgery. (E) Two months later, cranioplasty was performed. (F) In spite of severe left cerebral damage, she recovered dramatically. Now she can talk freely and play the piano.
|
She underwent DC, but brain swelling was so severe that dural closure was impossible. Despite the H-B therapy, her ICP was elevated up to 37 mmHg on the day after operation (Figure 2C and D). Reoperation, including removal of traumatic ICH, left temporal lobectomy, and internal decompression surgery, was performed. H-B therapy was continued for 5 days and did not cause any serious complications. Although severe damage was observed in the left cerebral hemisphere on CT after 2 months of injury (Figure 2E and F), the patients showed a marked recovery after the treatment. She can presently talk freely and play the piano. This recovery was a result of all the aforementioned treatments. It would be safe to conclude that this is an effect of the “All-in-One” therapeutic strategy.
Go to :
Results
Among the 439 patients transferred during this study, 158 required surgical treatments. Trepanation surgery was performed in the ER for 97 cases, and hematoma removal surgery and DC were additionally performed in the OR for 46 of these cases. Craniotomy surgery was performed in the OR as the first treatment for 61 cases whose neurological symptoms were relatively mild. H-B therapy was administered to 56 cases. Internal decompression surgery, including evacuation of traumatic ICH, was additionally performed for 12 cases, particularly for pediatric and young adult patients.
Three months after injury, the Glasgow Outcome Scale (GOS) score yielded the following results: good recovery in 25 cases (16%), mild disability in 28 (18%), severe disability in 33 (21%), persistent vegetative state in 9 (6%), and death in 63 (40%). Because many cases of a GOS score of ≤5 are included in this study, this result must be satisfactory. Moreover, certainly, neurologic symptoms present in many cases recovered subsequently. Forty-three (77%) of 56 cases treated with H-B therapy in addition to craniotomy in the OR were life-saving. Only 2 cases with trepanation surgery alone survived.
Notably, 27 patients (36%) of 76 most severe patients who had an abnormal response of bilateral eye pupils were lifesaving. In addition, 50% of the patients treated with internal decompression surgery recovered to the clinical condition wherein they could walk without assistance. Elderly cases (older than 75 years) predominantly showed poor outcomes (78%), and no one could return to their own home life.
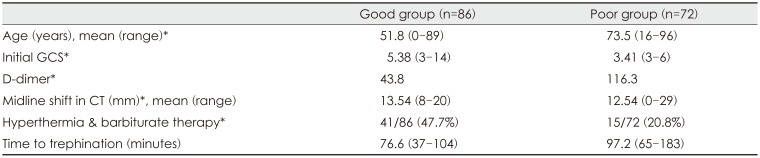
The differences in various parameters in the good and poor outcome groups are shown in Table 1. There were significant differences in the initial GOS score, age, and D dimer between these two groups.
Go to :
Discussion
How to achieve a rapid decompression treatment for TBI?
Despite the progress in modern medical technology, the outcomes of treatment for severe TBI remain poor.3142526) There is a therapeutic limit even if various treatments are administered in cases with extensive cerebral contusion, brain stem damage, or severe diffuse axonal damage as primary brain injuries at admission. In addition, some patients can be saved by minimizing brain swelling, but cerebral ischemia subsequently becomes a secondary brain injury after rapid reduction of ICP at initial stages.1151932)
Emergency craniotomy in the OR is the most effective method to reduce ICP markedly, but transferring patients to the OR immediately after admission is not always possible because every hospital has its common circumstances. In the most severe cases of impending cerebral hernia, there is a high risk of death and irreversible extensive damage to the brain, even if the time loss to treatment is only several minutes.511212428)
The first solution to this problem must be trepanation surgery in the ER. In our hospital, it takes 33.5 minutes on average to transfer patients for trepanation surgery. After the primary survey, trepanation surgery is performed by the neurosurgical team at the earliest to avoid irreversible traumatic brain damages. As more cases are treated in our hospital, communication and cooperation can be conducted smoothly between the emergency center staff and neurosurgeons, and trepanation surgery in the ER has become a routine first aid treatment.
The next step is DC in the OR. Although the effectiveness of DC in TBI is either limited or negative in previous studies,1018) DC is actually effective for controlling ICP.41229)
With respect to the technique of DC, not causing or releasing uncal hernia is of utmost importance. It is necessary to carefully consider its indication and timing. The initial steps in the series are to transfer patients to the OR and then perform DC after trepanation surgery in the ER, as stated in the principle policy.
Indeed, in many cases, the consciousness level was a GCS score of 3, and the examination of bilateral pupils revealed abnormal dilatation. Trepanation surgery in the ER showed no effect on more than 50% of these cases. Actually, in very severe patients, the survival rate could not be improved despite performing additional DC.23) Therefore, in the second half of the series, we did not perform additional aggressive DC treatment unless clinical symptoms did not improve after trepanation surgery, particularly in bilateral pupil abnormal cases.
Combined mild hypothermia and moderate barbiturate therapy
We developed H-B therapy 20 years ago and have practiced it not only in severe TBI cases but also in many cases of severe stroke.202122) The characteristic of this combined therapy is to use a mild treatment with deep body temperature control at 35℃ in combination with barbiturate therapy. Depending on disease severity, thiamylal sodium is used at 3 to 5 mg/kg/h. The duration of H-B therapy is 72 hours in general, but it can be extended to 120 hours in severe cases. Moreover, it is a widely known fact that stepwise slow re-warming is essential for TBI treatment. In contrast, rapid re-warming is associated with an explosive increase in cerebral metabolism and brain swelling.1317)
The reason for using these two powerful treatments together is to prevent the explosive brain re-swelling during the re-warming period. It is established that hypothermia therapy has many side effects. These adverse effects, such as pneumonia and hypokalemia, can be managed with intensive care. In fact, in some cases, explosive brain re-swelling occurred irrespective of how the gradual re-warming procedure was performed. In our experience, barbiturate therapy may suppress this adverse effect.
In recent clinical reports, hypothermia therapy has shown negative effects.289) However, basic research has revealed the protective effect of hypothermia therapy on TBI, and the protective mechanisms have been proven to have an inhibitory role in glutamic acid release,6) cerebral metabolism,31) and apoptosis.30) Therefore, the current situation is that the results of basic research are not consistent with those of clinical studies. In fact, only the negative aspects of hypothermia therapy are emphasized in these clinical studies, and clinical reports continueto deny the therapeutic effect of hypothermia therapy.289)
A randomized, multicentre clinical study (the National Acute Brain Injury Study: Hypothermia II [NABIS: H II]) concluded that this trial did not confirm the utility of hypothermia as a primary neuroprotective strategy in patients with severe TBI.9) However, the present findings need to be analyzed in detail. In the secondary analysis in the NABIS: H II study, the mortality rate was 27%, and favorable outcomes were 30% in the diffuse injury group. However, in the evacuated mass group, the mortality rate was 13%, and favorable outcomes were 67%. In addition, based on the Japan Neurotrauma Data Bank project 2009,27) the favorable outcome rate was significantly higher in hypothermia management than in normothermia management in the evacuated mass group. Therefore, hypothermia treatment shows obvious therapeutic effect in the evacuated mass group.
Why not stepwise strategy but “All-in-One” strategy?
In the treatment of malignant tumor, such as lung cancer, a multistage treatment algorithm is established. Based on the guideline, the first-line treatment must be performed, and the second-line treatments are optional and can be administered subsequently.
Should we treat severe TBI in this manner? The differences in the treatment between severe TBI and malignant tumor are obvious. As mentioned repeatedly, it is essential to make accurate and prompt decision because the delay of even several minutes for the treatment can cause cerebral hernia and result in traumatic death. If ICP control fails, it will take several hours to start the next stage treatment. In addition, if the next stage treatment must be performed after failure of the initial treatment, it will also take several hours to achieve the required effect. The important point to be emphasized is the time delay in the staged therapeutic protocol. In this situation, DC in the OR, hypothermia therapy, and barbiturate therapy have often been the next steps.2) The effectiveness of each treatment cannot be evaluated under such circumstances.
As mentioned at the beginning, accurate judgment and prompt action are essential to treat severe TBI successfully. A considerable number of clinical studies for severe TBI have been mainly designed based on stepwise treatment protocols.2) In general, the treatment will shift to the next step when the ICP management becomes difficult and uncontrollable. In the protocols, severe TBI is initially treated medically and then with external decompression, and hypothermia or barbiturate therapy is performed subsequently. Andrews et al.2) found that therapeutic hypothermia plus standard care did not result in better outcomes than did standard care alone in patients with an ICP of >20 mmHg after TBI.
Because this treatment is ineffective, is there a method to control ICP rapidly and effectively with a stepwise strategy principle? Time cannot be lost in protecting brain function while treating severe TBI. If an emergency DC surgery in the OR is decided, several tens of minutes will be wasted. Moreover, at least 1 and 2 hours are needed to obtain a therapeutic effect of mild hypothermia therapy. We cannot establish the same treatment policy as cancer treatment guidelines because a second-line anti-cancer drug can be used if the first line is ineffective. Indeed, we should not miss the “Golden Time” of treatment.5162128)
Another important aspect is that most TBI treatments are performed by young neurosurgeons and their judgment leads to entire and definite treatment decisions. Treatment of severe TBI requires prompt action. Therefore, delay in judgment, inappropriate decision, and hesitation for more aggressive treatment may result in miserable clinical results.
Here is another reason for conducting the “All-in-One” strategy. In this policy, effective treatments strategies are implemented at the earliest at the initial stages, and the best treatment is executed without any hesitation. The remained decision is about internal decompression surgery, although it is not necessary in the first stage of treatment.
Of course, this idea is accepted on the premise that serious complications can be overcome. Actually, serious complications never occur in our TBI patients because strict intensive care unit management has been ensured in our institution in recent years. To date, the negative effects of barbiturate and hypothermia therapy have been a main focus.289)
Cooperation with other experts
In the treatment for high energy trauma, such as traffic and fall accidents, coordination with other departments is very important. In Japan, before the JATEC initial clinical practice guidelines were developed and introduced, there were many cases called “Preventable Traumatic Death,” In particular, treatment for severe TBI was strongly emphasized at that time. However, because the primary survey policy was thoroughly obligated, the incidence rate of “Preventable Traumatic Death” has decreased markedly. The priority of the treatment for high energy trauma should be clarified. Tension pneumocephalus and retroperitoneal hemorrhage associated with pelvic fracture and traumatic cardiac tamponade should be prioritized. In addition, it will be ideal if the neurosurgical team and other department teams can perform procedures simultaneously. Actually, trepanation surgery for ASDH and therapeutic embolization for intraperitoneal bleeding can be performed simultaneously.
Limitations of the study
This clinical study has several limitations. First, this is a retrospective, and not randomized, study. Ideally, it is best to evaluate the effect of the “All-in-One” therapeutic strategy in a prospective randomized controlled study. Second, the neurological outcomes are defined at 3 months after the injury. However, young patients can recover in a year. In addition, TBI in elderly patients can worsen because of systemic complications in the chronic stage. Further studies, incorporating a larger number of patients with a longer follow-up time, are needed to confirm the efficacy of the “All-in-One” therapeutic strategy.
Go to :
Conclusion
This therapeutic strategy without any loss in the appropriate treatment timing can improve the outcomes of severe TBI cases. At present, complications associated with hypothermia and barbiturate therapy can be overcome, and all selectable treatments should be attempted in severe TBI cases. We think that the breakthrough in the treatment of severe TBI will depend on the shift in the treatment policy.
Go to :
 XML Download
XML Download