

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Technological advances in magnetic resonance imaging (MRI) have facilitated the diagnosis of spinal tumors. The most common intradural extramedullary tumors are schwannomas, neurofibromas and meningiomas and the most common intramedullary tumors are astrocytomas and ependymomas. Extradural lesions are most commonly metastatic neoplasms.8) However, it is difficult to distinguish spinal cord tumors using MRI.
As a result, surgical biopsy procedures are often performed on lesions.3) Here, we report a case in which the thickening ligamentum flavum (LF) appeared to be a tumor in the epidural space of the cervical spine based on imaging findings.
Go to : 
Case Report
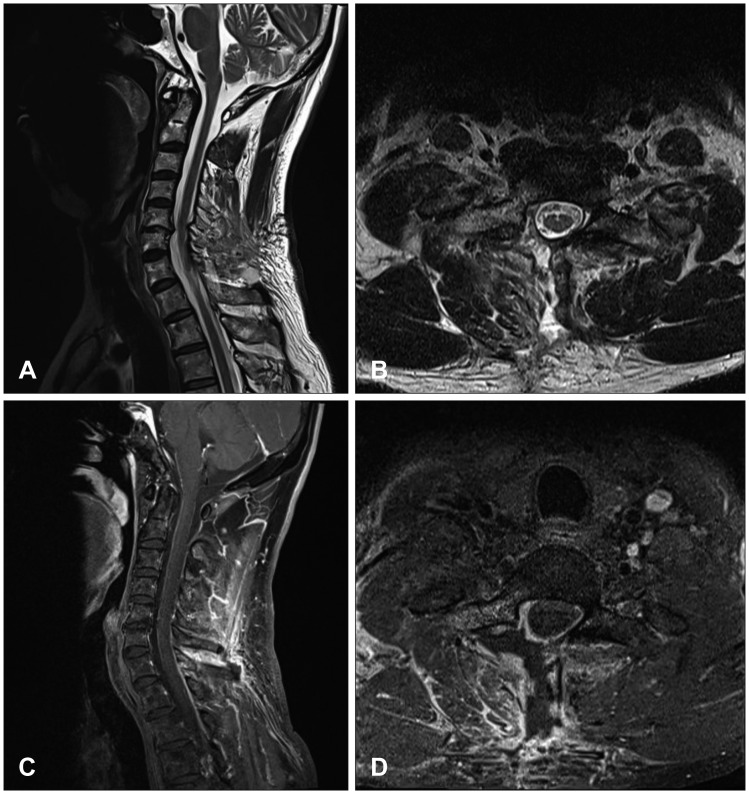
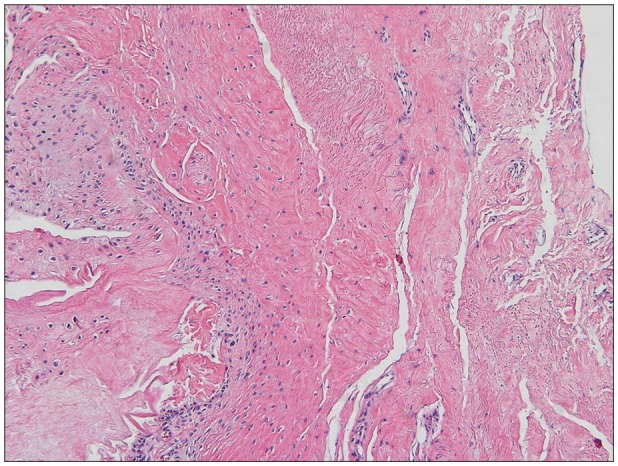
A 52-year-old man visited our clinic with severe shoulder pain and radicular pain (Numeric Rating Scale, 7) in his right arm that gradually worsened after a traffic accident 2 months ago. Upon admission, MRI of the cervical spine revealed an extradural mass, which was about 2.4 cm in size, with marginally high signal intensity on T2- and T1-weighted images with gadolinium, demonstrating an ill-defined, heterogeneously enhancing mass in the right epidural space at the C7-T1 level (Figure 1). We suspected a tumor, performed an operation to decompress the spinal cord, and obtained a biopsy of the mass. At the time of surgery, the LF was thick and compressed the spinal cord. We removed the LF very carefully by dissector and punch. After successful removal of the LF, the spinal cord appeared normal (Figure 2). Post-operative spinal MRI performed 1 week later showed no sign of compression of the spinal cord by mass effect (Figure 3). The results of the histopathological examination confirmed that removed mass was the LF. Histopathological examination also revealed elastic fibers with irregular arrangement, reduced elastic components, and increased collagen tissue (Figure 4). The patient was discharged without pain or weakness 2 weeks postoperatively. During 6-months of follow-up, there were no complications.
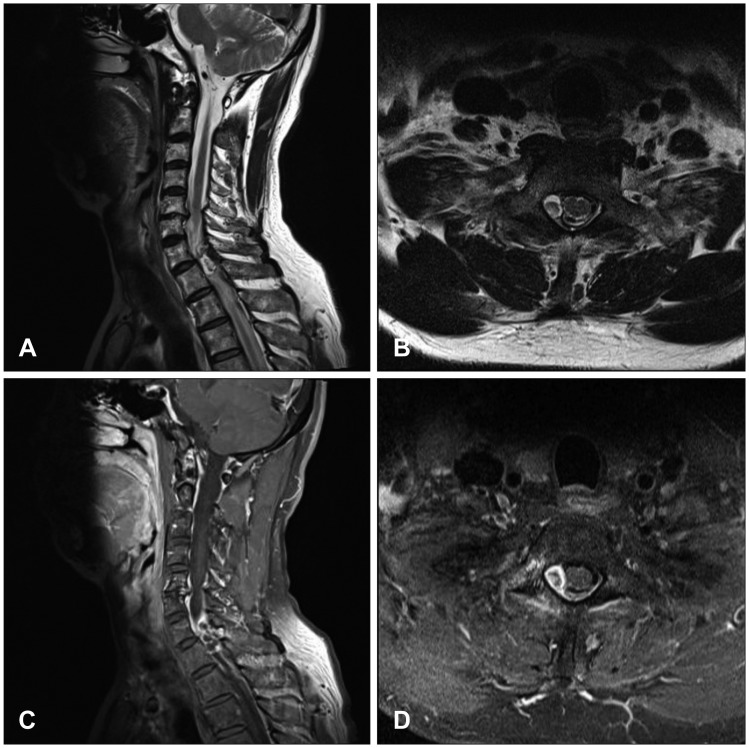 | FIGURE 1Preoperative T2-weighted magnetic resonance images (MRIs): (A) sagittal and (B) axial views. T1-weighted MRIs with gadolinium: (C) sagittal and (D) axial views. The images revealed an extradural mass at the right epidural space of the C7-T1 level.
|
 | FIGURE 2(A) Intraoperative photograph showing the hard and stiff epidural mass (arrow) compressed the spinal cord. (B) After careful removal of the epidural mass using a dissector and punch, the spinal cord appeared normal.
|
Go to :
Discussion
In spinal cord lesions, as well as in tumors, inflammation and infectious tissue can cause mass effects detected with imaging. In addition, we found that thickening of the LF may also induce mass effects to the spinal cord.
The LF is stiffer than other ligaments and prevents collision of the spinal cord during neck motion of the spine.2) However, the LF may encroach on the dura or cord by folding and bulging which may lead to clinical symptoms of radiculopathy or myelopathy in the extension position.7) Zhong et al.9) reported a retrospective analysis of kinematic MRI that may reveal LF bulging and spinal cord collision. We assumed that microtrauma due to repetitive movements such as flexion and extension could thicken the LF over time. Thickening of the LF is generally known to occur due to buckling on the spine. Published papers have reported that fibrosis is the main cause of LF hypertrophy, and is caused by the accumulation of mechanical stress due to aging.145)
Furthermore, the cervicothoracic junction is a transition zone between the mobile lordotic cervical spine and the rigid kyphotic thoracic spine. Biomechanical forces and structure predispose the cervicothoracic junction to increased loads that can potentiate instability. For this anatomical reasons, we can expect the LF at the C7-T1 level will be thicker than at other cervical levels. Sayit et al.6) reported that the mean thickness of the LF depends on cervical level and patient position, and the LF at the C7 level is significantly thicker than that at other levels. Therefore, it is likely that if the LF at the cervicothoracic junction has thickened, it may be perceived as a tumor in the cervical spine.
In our case, thickening of the LF should be considered a possible etiology of the extradural mass. Also, decompression surgery is needed to relieve the symptoms caused by the mass effect and a diagnosis must be confirmed as early as possible. In the present case, although a decompression operation was performed due to misdiagnosis of the tumor, early surgical intervention showed favorable results without neurological deterioration.
Go to :
Conclusion
We report a case in which the thickening LF appears to be a tumor in the epidural space of the cervical spine based on imaging findings. In our case, it is likely that the LF at the cervicothoracic junction has thickened, and it is perceived as a tumor of the cervical spine that compresses the spinal cord.
Go to :
 XML Download
XML Download