

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Decompressive craniectomy (DC) is a traditional, classic and evidence-based surgical method for intractable increased intracranial pressure not responding to medical treatments. Cranioplasty after DC with a patient's autologous skull flap is a worldwide practice.554) The increase of DC leads to an increase of cranioplasty.12)
According to the open data from Healthcare Big Data Hub, which is provided from Health Insurance Review and Assessment Service of Republic of Korea, approximately 1,900 patients have received cranioplasty annually between 2010 and 2015 (Table 1).
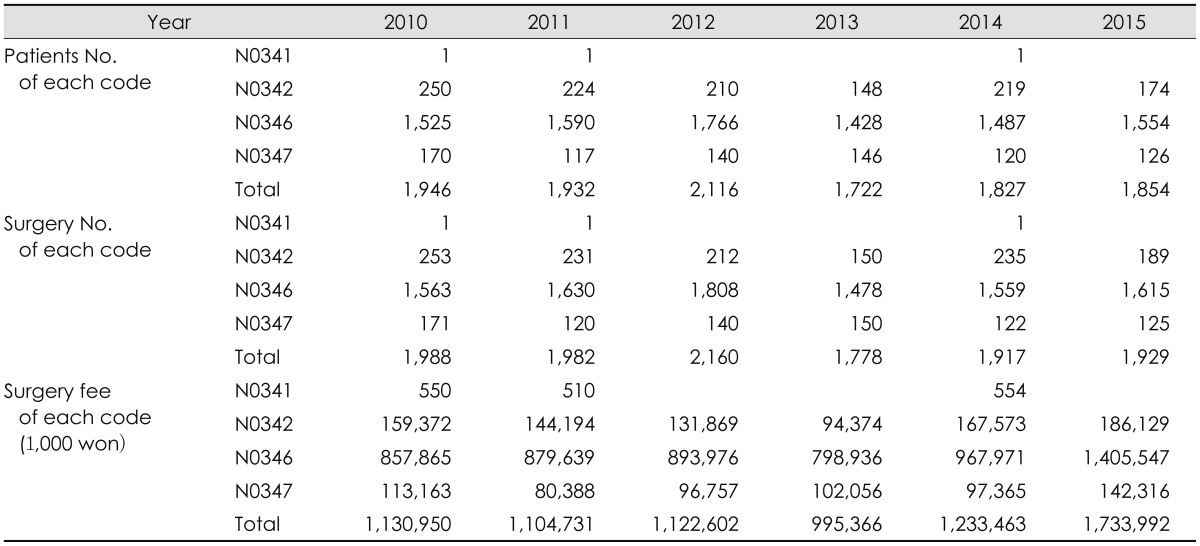
TABLE 1
Open data of cranioplasty from Healthcare Bigdata Hub which is provided from Health Insurance Review and Assessment Service, Republic of Korea. Cranioplastys for craniosynostosis are excluded. Code N0341 means simple cranioplasty limited in skull, N0342 means cranioplasty including duroplasty, N0346 means relatively simple cranioplasty and N0347 means relatively complex cranioplasty. Surgical fee was increased with phase-out of the selective medical fee in 2014 Jul in Repubic of Korea
![]()
There are many reports about cranioplasty in literatures such as case series, case-control study, cohort studies, clinical trials and complications data. Major topics on cranioplasty are such as complications, surgical timing, surgical technique, free flap preservation methods, new materials and cost-effectiveness. In a few references, there are efforts to provide and support biological basis for cryopreserved bone flaps.7192841)
In this report, we want to review current information on cranioplasty from the purpose of cranioplasty to the cost-effectiveness of new materials and techniques.
Go to : 
Objectives of Cranioplasty
The reason we should perform cranioplasty after DC is to protect the brain, achieve a natural appearance and prevent sinking skin flap syndrome (or syndrome of the trephined). Furthermore, cranioplasty may improve neuronal function. Many literatures report cranioplasty enhances cerebral glucose metabolism, cerebrovascular reserve capacity, postural blood flow regulation and cerebrospinal fluid circulation.111217)
Go to :
Optimal Timing of Cranioplasty
The optimal timing for cranioplasty remains a controversial topic.11) One author reported 390.4 days as the mean time between craniectomy and cranioplasty in 2015.39) Some authors have defined “early cranioplasty” as cranioplasty less than 91 days after craniectomy.3756) In Korea, if the patient's condition is favorable, the timing of cranioplasty can be shortened to less than six weeks following DC.1453) Optimal timing of cranioplasty is thought to be related with cranioplasty complications. The most important complication of cranioplasty is postoperative infection. There are several risk factors such as operation time exceeding 90 minutes, early cranioplasty, patient's age older than 20 years, female patient, and so on.12) In the past, delayed cranioplasty was considered the optimal timing because it showed a lower infection rate.43) Many authors reported cranioplasty before six months after craniectomy was associated with poor outcomes.43) Tasiou et al.51) reported delayed cranioplasty preference is associated with efforts to decrease postoperative infection, especially for traumatic brain injuries. Recently, several reports recommend early cranioplasty, because it was found that cranioplasty improved clinical outcomes.364247) In the aspect of postoperative infection, multinational prospective designed study says no difference exists of the infection rates between early and delayed cranioplasty.42) In meta-analysis, there was no difference in the chances of developing postoperative infection between early and late cranioplasty.37)
Go to :
Autologous Skull Flap
Autologous bones are cost-efficient and cosmetically natural.34) In general brain surgeries, skull flaps are usually re-inserted and strong bony fusions between bone flaps is achieved. This is natural because osteogenic, osteoinductive and osteoconductive materials are rich in fresh bone flaps.
Transplanted bone flaps undergo complex healing processes to fuse with surrounding bones.45) Capillary invasion and osteoblasts migration from surrounding bones are important for the bone flap's survival. After re-implantation, no blood is supplied to the bone flap, leading to ischemia. The bone flap is surrounded by blood and an inflammatory response is initiated. Capillaries from surrounding bone, dura and periosteum initiate angiogenesis to the bone flap. As granulation tissue proliferates, capillaries invade the flap. Through the capillary, primitive mesenchymal cells migrate and bone remodeling occurs. Necrotic bone is gradually reabsorbed. If this functional contact between the transplanted flap and surrounding bone is poor, the transplanted flap will be absorbed.45) In animal studies, free skull flaps showed a 50% reduction in volume after re-implantation.18) Similarly, an experimental study on particulate bone on-lay cranioplasty also showed that half of the on-lay graft was resorbed.15)
Fresh skull flaps should be preserved sterilely after DC. There are two methods to make autologous skull flap sterile for cranioplasty: subcutaneous layer placing or cryopreservation.14273238)
As the deep-freezer freezing technique developed, cryopreservation became a more economic and practical method.16) However, there is not a lot of information on how to cryopreserve skull flaps. Bhaskar et al.8) reported 96% of 25 neurosurgical centers in Australia used cryopreserved autologous bone flaps for cranioplasty. In his report, 88% of institutions used double or triple gabbed under dry, sterile conditions for packing bone flaps. The bone flaps were cryopreserved at temperatures between -18℃ and -83℃.8) Biomechanical studies reveal that freezing and thawing have little effect on the mechanical properties of the human skull.54) Sometimes, autoclave or ethylene oxide gas sterilization techniques were used for preventing postoperative infection.263846) However, biological evidence of cryopreserved cranioplasty is obscure. There are few reports on the osteogenic potential of cryopreserved skull flaps. It has been reported that osteoblasts were not cultured from skulls cryopreserved for more than 6 months.7)
Go to :
Bone Substitute for Cranioplasty
If a skull flap was suspected of contamination, the bone flap would be disposed of. Traumatic brain injuries with a severely contaminated wound or a bacteria-infected wound should undertake delayed cranioplasty with synthetic materials. The ideal synthetic material should be easy to shape and should accurately fit skulls with a cranial defect. The material should be radiolucent enough to avoid formation of artifacts on images and biocompatible to lessen immune response or inflammation. It should be firm and stable, resistant to infection, heat and cold. Finally, it should be economical.329)
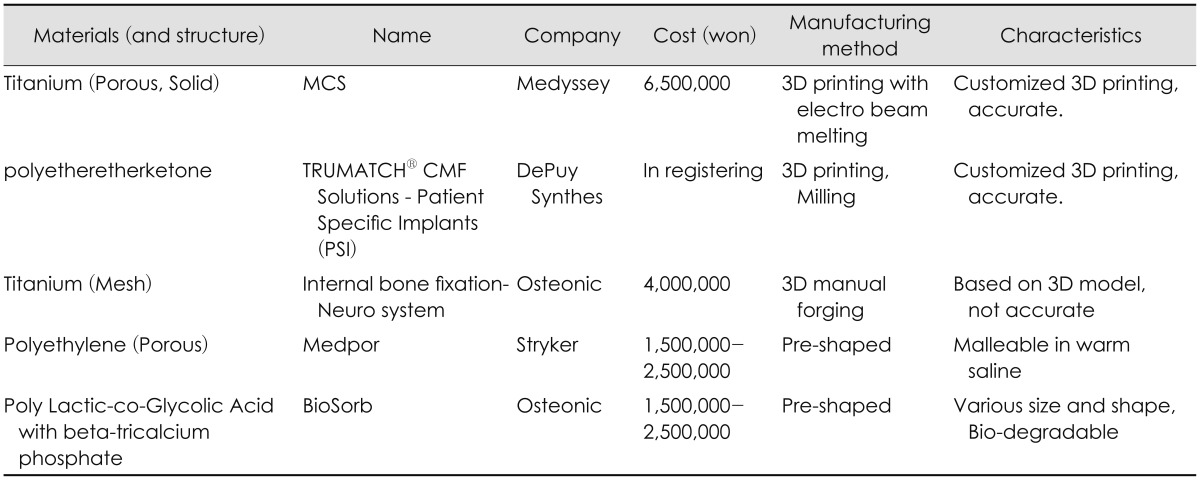
Various materials are used as synthetic materials such as metals (titanium, tantrum etc.), ceramics (calcium phosphate, hydroxyapatite etc.) and polymers (Polymethyl methacrylate [PMMA], polyethylene, poly-ether-ether ketone, poly-ether-ketone-ketone, etc.), bioactive fiber-reinforced composite, demineralized bone matrix and so on.3934353940) Recently, custom-made prostheses for cranioplasty printed with three-dimensional printers are on market (Table 2, Figure 1).48)
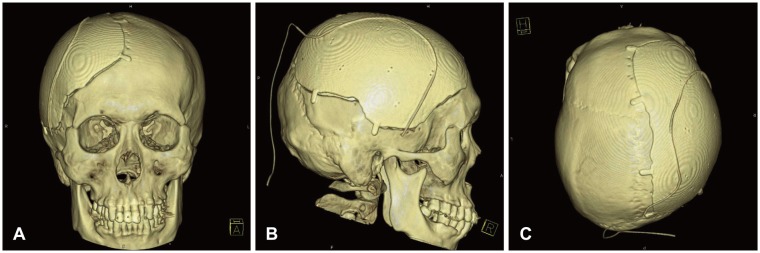 | FIGURE 1Brain computed tomography (CT) three-dimensional (3D) reconstructions after cranioplasty with Titanium skull flap. Bone flap is made by 3D printing with electron beam melting technique. Pre-craniectomy brain CT and pre-cranioplasty CT were used for tailored flap. Subgaleal drain catheter is seen above metal flap. (A) Frontal view, (B) Right lateral view, and (C) Apical view.
|
Go to :
Special Surgical Considering for Periosteal-dura Mater Dissection
Dissecting the dura mater and the scalp-muscle flap is a difficult process during cranioplasty. Temporalis muscle injury may result in pain and dysfunction of masseteric action. For this reason, some authors support early cranioplasty within one month before adhesion becomes firm. Some authors recommend using anti-adhesives like artificial dura mater or film to facilitate dissection, and some authors recommend new dissection plane.142122)
Go to :
Antibiotics on Surgical Field
Antibiotics preventing post-cranioplasty infection were used clinically. However, PMMA impregnated with antibiotics, preoperative prophylactic vancomycin for Methicillin-resistant Staphylococcus aureus (MRSA) and prophylactic vancomycin ointment at the cranioplasty site shows low grade evidence.25434455)
Go to :
Complications after Cranioplasty
The overall complication rate for cranioplasty after DC was 10% to 40%.253) These complications include infections, reoperations, intracranial hemorrhage, extra-axial fluid collection, hydrocephalus, seizures and bone resorptions.37)
The most well-known complications are postoperative surgical infection and bone flap resorption.49) The bone flap infection rate after cranioplasty was 2% to 20%.253) Risk factors include long operative times (>120 min), craniectomy with temporalis muscle resection, and presence of preoperative subgaleal fluid collection(s), and postoperative wound disruption.30) Fever, scalp swelling and local inflammations were presented. Imaging study shows extra-axial fluid collection, subgaleal fluid collection, galea swelling, cerebritis, osteomyelitis, and so on.6) In bone flap culture during surgery, primary skin flora such as P. acnes, coagulase-negative staphylococci and S. aureus were cultured.13) However, P. acnes, Escherichia coli, MRSA and S. aureus are among the pathogens identified in surgical site infection (SSI) after cranioplasty.49) Generally, patients that developed SSI were treated with antibiotics following antimicrobial susceptibility testing for 4 to 8 weeks after removal of the implanted bone.
Bone resorption indicates bone tissue resorption by osteoclast, which breaks down bone tissue and releases minerals from bone tissue to the blood.52) Resorption after cranioplasty means decreased bone volume or bone mineral density after autologous cranioplasty. The reported rates were between 2.7% and 44.4%. Computer tomography was used for bone resorption diagnosis. There is a report using computed tomography house field unit scores for resorption diagnosis. Children and large skull flaps, long cryopreservation periods, fragmented flaps and Glasgow Outcome Scale at the time of cranioplasty were reported as risk factors.103337)
Go to :
Cost Effectiveness of Autologous Skull Flap in Korea
Many researchers emphasize the economic merit of cranioplasty with autologous bone flaps.233435) There are many reports about new substitutes. The difference of the clinical outcome between synthetic materials and autologous bone graft in cranioplasty is very small.3435394048) Some authors report lower complication with synthetic materials.825262728) Some reports say the total cumulative cost, including complication risks and treatments, was not significantly different between titanium and autologous bone flaps in United States of America & Canada.2450) The total average cost of cranioplasty was $25,000 to $29,000 at Canada, reported in 2015.20) The medical environment of each country is different. The surgical fee of cranioplasty and the cost of synthetic materials are also different, even in Korea (Table 1). Following the development of science and industry, the total cost also is becoming more variable.
Up to this time, autologous cryopreserved bone flaps are the most ideal substitute for cranioplasty. Autologous bone flaps are valuable in two aspects. First, biologically cryopreserved skull flaps are the best scaffold for autologous osteoblasts. In the concept of tissue-engineered constructs, cryopreserved skull flaps are filled with osteoconductive and osteoinductive materials, which were completely matched immunologically with the recipient.31) Second, skull flaps are economic; there are no further costs.
Go to :
Conclusion
Cranioplasty after DC is a familiar surgical process to neurosurgeons. It is an essential surgery not only to satisfy patients' external defects, but also to improve patients' functional outcome. It is probable that many complications will arise because patients are in an immune-compromised state. New synthetic materials and techniques are introduced, and surgical results will also be improved clinically.
Go to :
 XML Download
XML Download