

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
In Seoul, the capital of South Korea, the occurrence of drowning after falling from bridges over Han River has increased. It is well known that falling from high-altitude bridge, such as the Golden Gate Bridge in San Francisco (about 67 meters above water), had very high mortality rates due to severe traumatic injuries.2346) The altitudes of bridges over Han River were medium-height, from 18 meters to 22 meters, and few reports have analyzed the injury characteristics of these patients. In the present study, we examined the injury patterns associated with these victims who jumped or fell from bridges over Han River.
Go to : 
Materials and Methods
Medical records of all drowned patients who were hospitalized in our institute between January 2011 and December 2015 were analyzed. We also collected the list of patients who had a history of falling from bridges over Han River.
Simple X-ray and computed tomography (CT) scans were performed. Chest and abdomen CT scans used contrast media, while brain and spine CT scans did not use any contrast media. Not all patients had a complete radiographic examination due to hemodynamically unstable state or refusal by the patient or guardians.
Injury Severity Score (ISS) was calculated for patients who had no cardiopulmonary resuscitation (CPR) or recovered spontaneous circulation after CPR. ISS was derived from the 2008 Abbreviated Injury Scale.5)
Go to :
Results
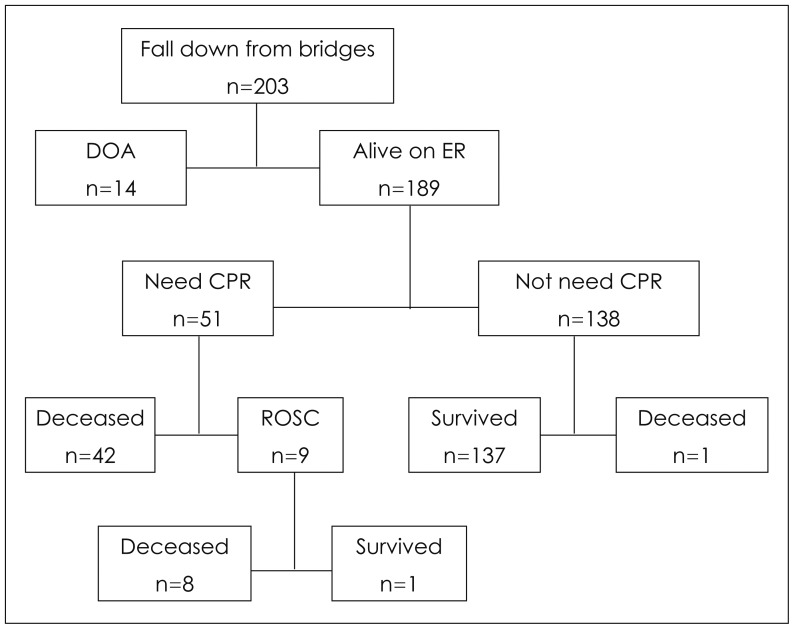
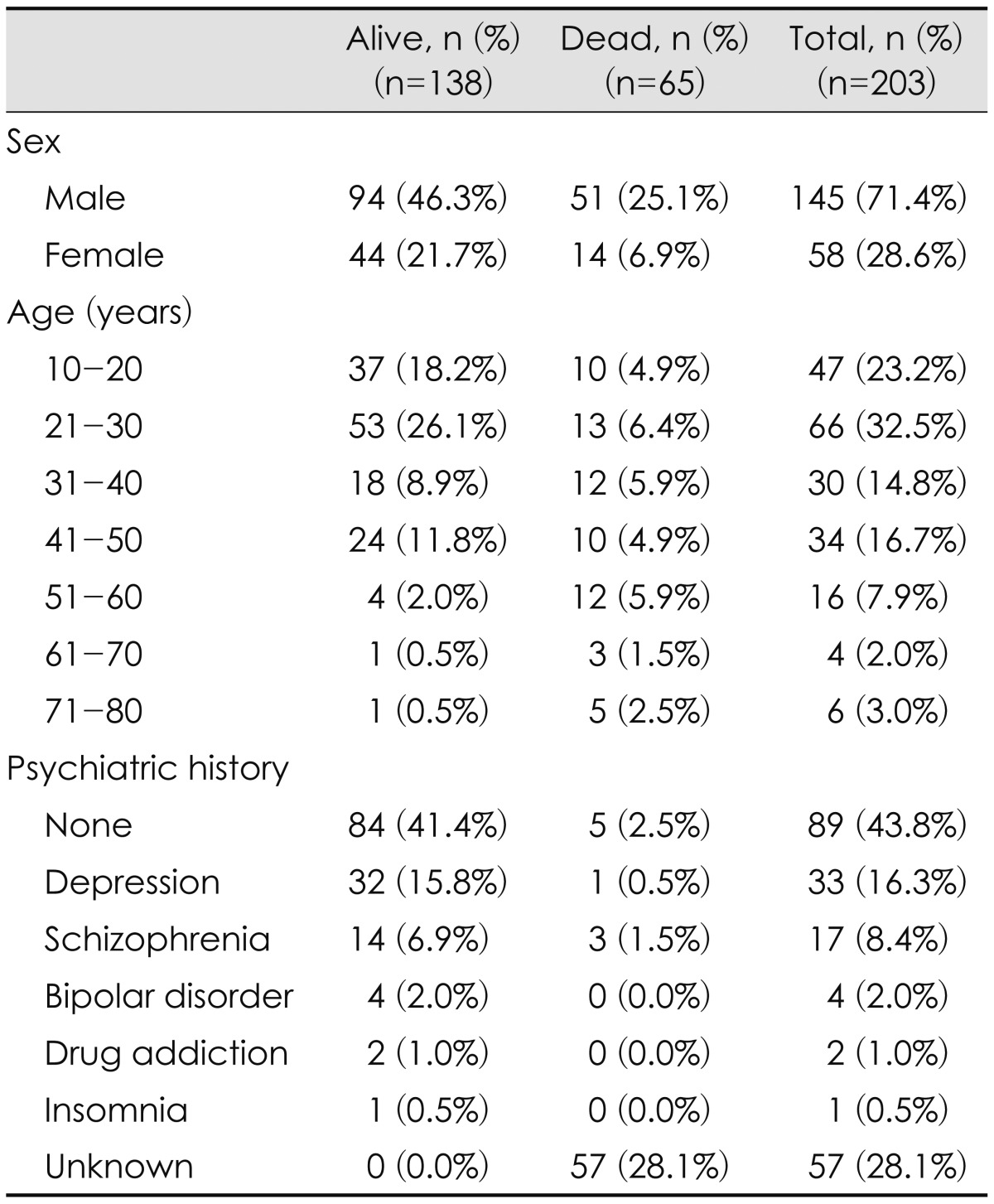
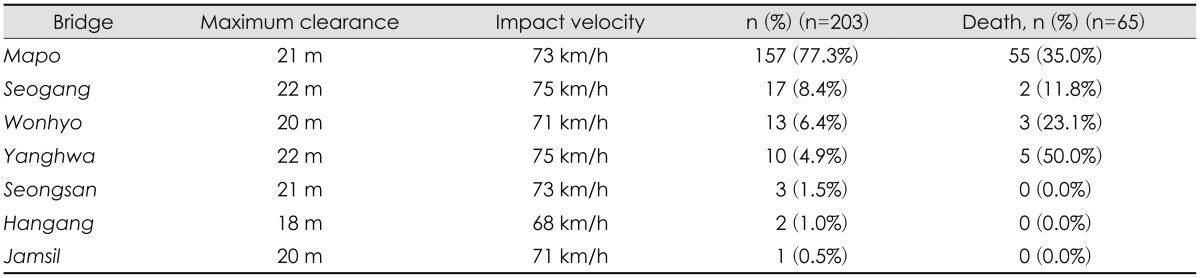
A total of 203 patients were transferred to our institute due to falling from bridges over Han River. The demographics of these patients are summarized in Table 1. The names of bridges and their characteristics are summarized in Table 2. Fourteen patients were already dead on arrival (DOA). Therefore, there was no evaluation for these patients. Immediate CPR was performed for 51 patients. Among these patients, only nine were recovered spontaneous circulation. Among patients for whom CPR was unnecessary, only one expired during treatment. A flowchart depicting the overall outcomes of these patients is shown in Figure 1.
Radiographic findings
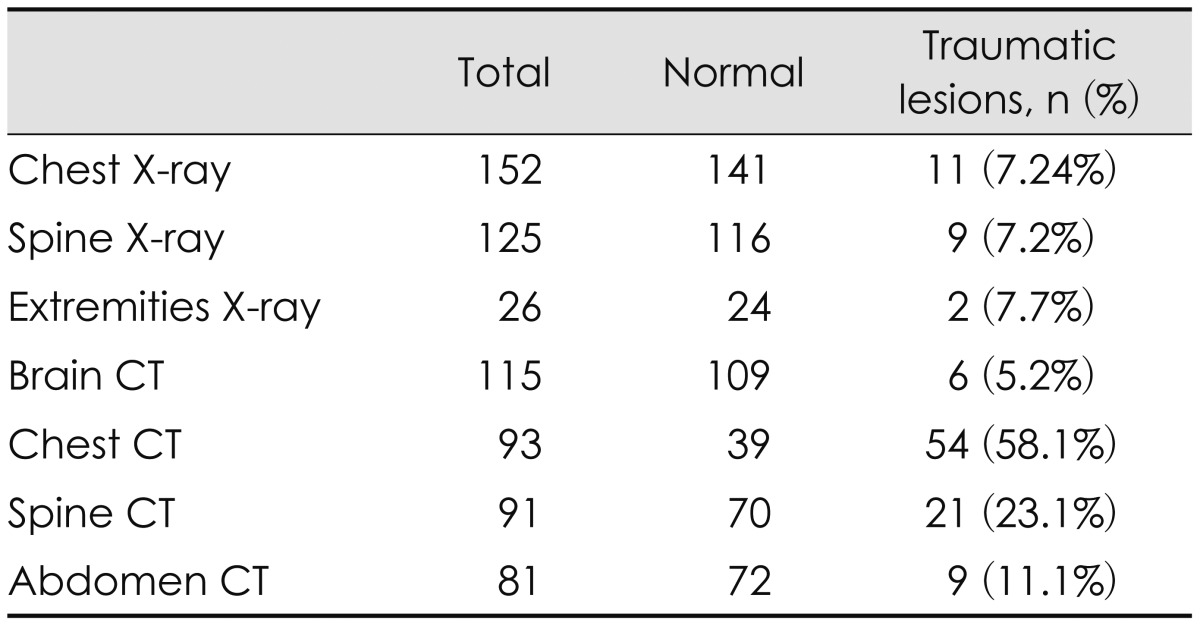
Except DOA patients and four patients who refused any evaluation, 185 patients underwent radiographic examinations. Of these, 141 patients underwent CT scans over one part. Traumatic lesions were identified in 96 (51.9%) patients. Radiographic data are summarized in Table 3.
Rib fracture was identified in four chest X-rays (CXRs). Seven CXRs revealed lung contusion. Five CXRs revealed pneumothorax. Fractures were identified in nine spine X-rays (one in the cervical spine, three in the thoracic spine, and four in the lumbar spine). Two extremity X-rays revealed one fracture on the metacarpal and one on the fibular bone.
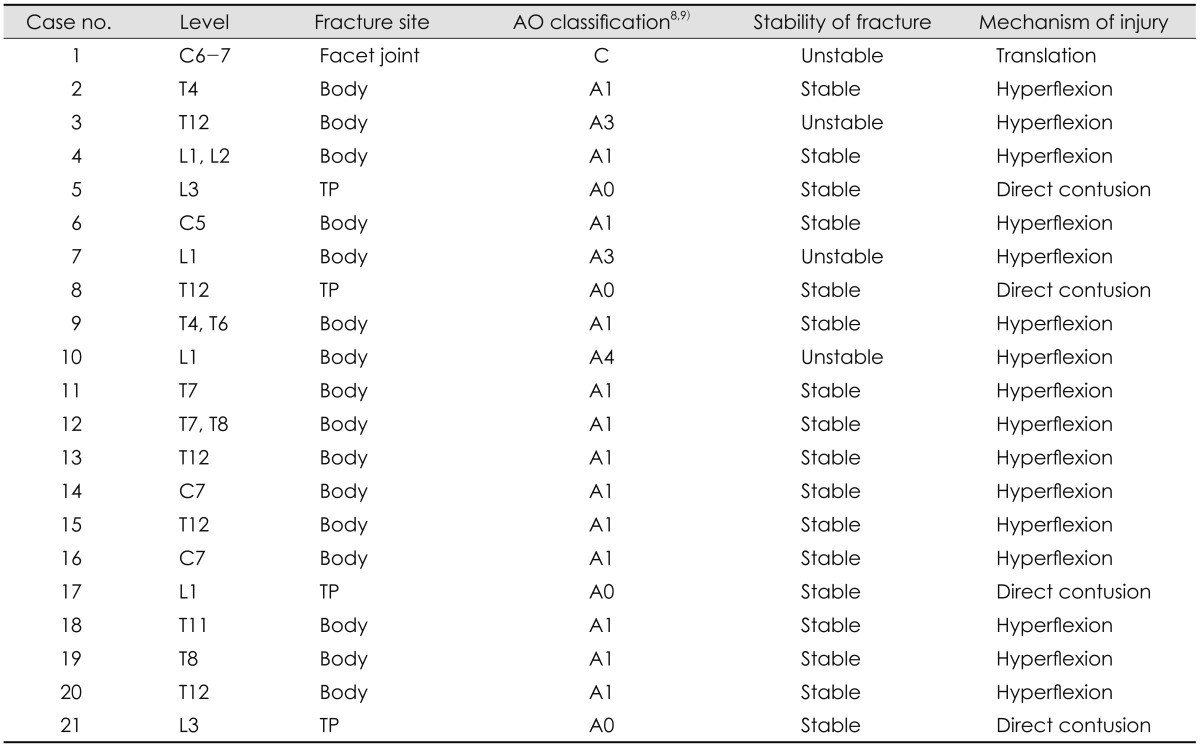
Six brain CT scans showed traumatic lesion. All findings were diffuse brain swelling. There was no focal injury, such as fracture or hematoma. In chest CT, rib fracture was identified in six CT scans while lung contusion was identified in 38 CT scans. A total of 19 CT scans revealed pneumothorax. Three CT scans revealed pneumohemothorax. In spine CT, unstable fractures were identified in four patients (one on the cervical spine, one on the thoracic spine and two on the lumbar spine). The others were stable (three in the cervical spine, ten in the thoracic spine, and four in the lumbar spine). All spine injuries were listed in Table 4. In the abdomen, liver injuries were found in five CT scans, spleen injuries were found in two, and adrenal gland injury was found in one. One abdomen CT scan revealed large hematoma needing exploration.
ISSs
The ISSs could be calculated for 147 patients. The mean ISS was 7.12±7.16. The minimum score was 3 points (no injury). The highest score was 45 points. 12 patients were classed as major trauma with ISS over 15, including 8 patients who were dead. The mortality rate of patients with major trauma was 66.7%. Among patients for whom CPR was unnecessary, only three were classed as major trauma. They had relatively good outcome.
Clinical outcome
The overall mortality rate was 32% (65/203) due to drownings after falling from bridges over Han River. Nine patients who needed CPR were recovered to spontaneous circulation. Therefore, the recovery rate of CPR was 17.6%. Among these nine patients, only one survived who was at vegetative state at discharge. The survival rate was 1.96% after CPR.
Among 138 patients for whom CPR was unnecessary, eight patients (5.8%) needed interventions (chest tubing in four patients, spinal instrumentations in two patients, intraabdominal hematoma removal and bleeding control in one patient, and internal fixation for metacarpal fracture in one patient). Most patients had good outcomes. However, one patient was at vegetative state at discharge. This vegetative patient had brain CT finding of diffuse brain swelling due to hypoxia. One patient died from fat embolism after a surgery to stabilize the fractured spine.
Go to :
Discussion
Several articles have reported the jumping or falling into the water from bridges. Trauma patterns of jumping from higher bridges include rib fracture with penetration, lung injury, and liver and spleen injury attributed to the impact.47) It has been reported that skeletal trauma among suicidal bridge jumpers is focused in the thorax and craniofacial regions, but less frequent in vertebrae and extremities.1) However, in our study, bridges over Han River have medium heights. The mean height of these bridges was 20.5±1.4 meters. Few articles have reported injuries due to falling from medium height bridges. Heming et al.3) have stated that there is no study about injuries associated with falling from a bridge whose height does not exceed 22 meters. Clinical articles reporting injuries associated with falling from medium height bridges are summarized in Table 5.

The mortality and injury rate of our study were different from those of previous studies. In the study of Heming et al.3) the mortality rate was higher than other series. The reason may be due to patient population. Heming et al.3) only included patients with cardiac arrest due to drowning. Therefore, the mortality in their study was very high. Their injury rate was similar to that in our study. On the other hands, in Brice et al.'s study2), the injury rate was low than other series. In their study, the mean height of bridges was low. They did not mention spinal and intraabdominal traumas. These might be associated with a low injury rate.
Our patients had injuries to their chest the most frequently. However, severe traumas on the chest were rare. The incidences of liver or spleen injuries were relatively less frequent, whereas spine traumas were more frequent than intraabdominal organ injury. However, unstable fractures needing stabilization surgery were rare. On the other hands, traumatic lesions at brain CT scans accounted for a small part of total injuries. However, the degrees of severity were very high. Only two patients with diffuse brain swelling were alive, and they were vegetative state at discharge. The rate of severe multiple traumas with ISSs over 15 was 8.2% (12/147).
The reason for the high incidence of thoracic and spinal trauma is unclear. The depth of Han River is deep. Therefore, there is no direct trauma to bottom of the river. Most of impact is caused by hitting the surface of water. Thus, the greatest impact would be transmitted to the human trunk, which occupies a large area and a heavy weight. It is thought that this causes high incidence of trauma on the thorax and the spine.
In our series, the cause of death could not be analyzed. The reason might be that autopsy was not performed routinely in South Korea. In addition, jumping or falling from the bridge occurred intentionally rather than accidentally.10) In general, many guardians and close relatives hope to downscale the aftermath of the accident and did not want the autopsy. The major cause of death among patients who were drowned after jumping or falling from the bridge had been known as asphyxia. Therefore, the proportion of severe trauma was low.123) In the same manner, we believed that asphyxia during drowning is the main cause of deaths, because general severities of injuries are low in our study.
This study had several limitations. First, it was a retrospective study. There was no routine protocol to evaluate these patients. Therefore, radiographic examinations were not uniform. Second, we might not have identified all jumpers or falling from bridges over Han River. Especially, some patients who looked appeared be less injured might have been transferred to the nearest secondary hospital from the drowning site.
Go to :
Conclusion
People who jumped or fell from bridges over Han River had high mortality rate. Among survivors, skeletal traumas were frequently encountered. Trauma patterns were concentrating on the thorax and spine regions. Therefore, complete radiographic evaluations including thorax and spine region should be performed for these patients.
Go to :
 XML Download
XML Download