

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Severe fever with thrombocytopenia syndrome (SFTS) is an infectious disease caused by the SFTS virus (SFTSV; family Bunyaviridae, genus Phlebovirus).13) It was first identified in rural areas of central China in 2009, and is thought to be transmitted by the tick species Haemaphysalis longicornis. The distinguishing clinical features of SFTSV infection are high fever accompanied by thrombocytopenia, leading to multi-organ failure.5)
The clinical course of SFTS can be divided into three major stages starting with fever, followed by multi-organ dysfunction, and then convalescence.9) The fever is typically accompanied by thrombocytopenia, gastrointestinal symptoms, and leukocytopenia.3) The initial investigation reported a fatality rate of 30%, however due to improvements in diagnosis and treatment, a recent study reported a fatality rate of 12.2%. Most fatalities are caused by hemorrhage or multi-organ failure.514)
A recent study reported that 19.1% of 538 SFTS cases also had encephalitis, and that 44.7% of these patients died.2) But there have been no reports of SFTS cases with intracranial hemorrhage such as subdural hemorrhage (SDH), epidural hemorrhage, and intracerebral hemorrhage (ICH). In this study, we report an extremely rare case of spontaneous acute SDH occurring in a patient with SFTS.
Go to : 
Case Report
The case is a 79-year-old farmer who lived in the countryside of a southern province in South Korea and was on medication for hypertension and hypothyroidism. He had no known history of food or drug allergies. He was admitted to a hospital in Seoul, with referral from a local clinic after 1-week of conservative care for fever. His wife was admitted to another hospital for fever with suspicion of SFTS.
Clinical history
The patient had a sustained fever (up to 38.9℃) with chilling, myalgia, and headache for 1 week while at a local hospital. He received antibiotics, but there was no clinical improvement. He was transferred to the hospital in Seoul with fever, myalgia, nausea, and diarrhea. A tick-borne disease or lymphoma was suspected. He was initially treated with intravenous Maxipime. The day after admission, he was given intravenous teicoplanin, ribavirin, and other supporting agents. On the third day of hospitalization, his mental state changed from stupor to semi-coma, with both pupils dilated (6 mm fixed). Emergent brain computed tomography (CT) indicated bilateral acute SDH. The hemorrhage was mainly on right fronto-temporo-parietal area, but a small amount was on the left cerebral convexity. He underwent emergency decompressive craniectomy. During the operation, his brain was pale, tense, and pulseless, and had a fungating lesion. With appropriate supportive care, he was stabilized but never returned to alert mentality. He expired 43 days after admission to our hospital due to cerebral dysfunction despite our extensive efforts.
Laboratory investigations
Laboratory tests indicated thrombocytopenia, hepatic dysfunction, and a high LDH level. Over time, the thrombocytopenia and hepatic dysfunction tended to become less severe, but the LDH level remained very high (Table 1). In particular, the initial platelet level was extremely low, inducing bilateral conjunctival hemorrhage. On day 3, progressing multi-organ failure was indicated by elevated liver enzymes (alanine aminotransferase [ALT] and aspartate aminotransferase [AST]) and lactate dehydrogenase (LDH). The thrombocytopenia was corrected by transfusion. After decompressive craniectomy, the laboratory findings stabilized over time. During hospitalization, there were no abnormalities of prothrombin time (PT) or activated partial thromboplastin time (aPTT).
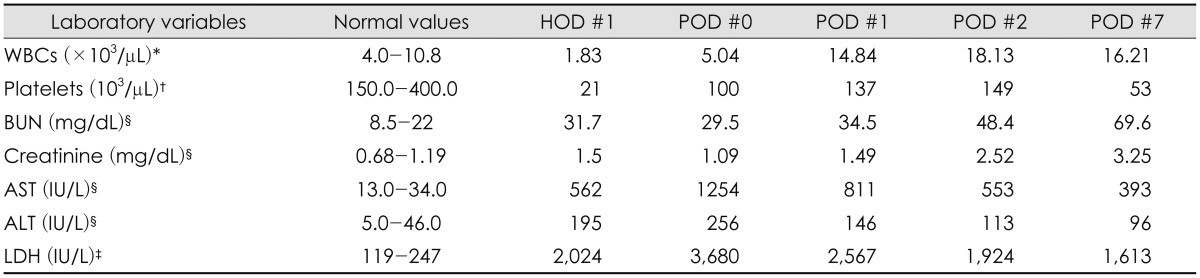
TABLE 1
Serial laboratory findings of the patients
*values indicate leukopenia, †thrombocytopenia, ‡elevated LDH level, and §multi-organ failure, all signs of severe fever with thrombocytopenia syndrome. WBCs: white blood cells, BUN: blood urea nitrogen, AST: aspartate transaminase, ALT: alanine transaminase, LDH: lactate dehydrogenase, HOD: hospitalization day, POD: post-operative day
![]()
After surgery, blood samples were sent to the National Research Institute of Health, Republic of Korea and were confirmed as positive for SFTSV by real-time reverse transcription-polymerase chain reaction (RT-PCR) analysis (Specimen Number SVS0020). PCR tests for other pathogens, including Chlamydophila pneumoniae, Mycoplasma pneumoniae, Legionella pneumophila, Bordetella pertussis, Bordetella parapertussis, and Parvo B-19 virus, were all negative.
Radiography findings
The first brain CT was taken on the day of admission to rule out central nervous system (CNS) involvement because of the patient had mental confusion. The results indicated no evidence of hemorrhage or inflammation, such as encephalitis, and no brain swelling, with intact sulci markings and ventricle size. The next brain CT, taken after a change in the patient's mental state (day 3 after admission), indicated a massive and prominent acute SDH on the right convexity of the brain. There was definite midline shift to left side and effacement of sulci markings, consistent with extensive brain swelling, although white matter and gray matter were distinguishable. After decompressive craniectomy, a post-operative CT indicated the brain had swollen severely, and shifted to the right side, a devastating outcome. The CT finding was consistent with brain herniation, white matter and gray matter were indistinguishable, and ICH and spontaneous subarachnoid hemorrhage were observed (Figure 1).
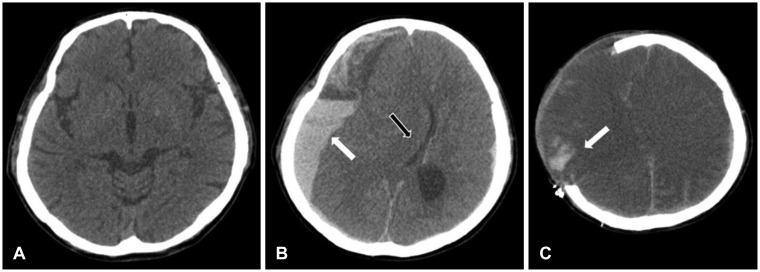 | FIGURE 1(A) Initial computed tomography (CT) scan taken in the emergency room upon admission to our hospital, indicating no abnormal findings. (B) Preoperative CT scan (day 3 after admission to our hospital) indicating a massive acute subdural hematoma on the right cerebral convexity with effacement of sulci markings (white arrow) and a midline shift (black arrow). (C) Postoperative CT scan showing intracerebral hemorrhage (white arrow) and devastating brain swelling.
|
Go to :
Discussion
SFTS is novel febrile disease that was first reported in central China. An investigation of this disease in 171 patients led to the identification of a new virus, SFTSV.9) This species constitutes a third group within the Phlebovirus genus of the Bunyaviridae family. A previous study collected SFTSV RNA from some ticks in the Ixodidae family of the species Haemaphysalis longicornis that were on domestic animals.13) Tracking of disease progression in 59 SFTS cases led to identification of 3 stages of SFTS: fever, multi-organ dysfunction (MOD), and convalescence. Thus, SFTS patients initially suffer from flu-like symptoms, such as fever, myalgia, and headache. Gastrointestinal symptoms and lymphadenopathy are also very common at this stage. On average, this stage persists for approximately 7 days and is accompanied by leukopenia and thrombocytopenia. The MOD stage, according to the diagnostic criteria of MOD, develops rapidly at 7 to 13 days after the onset of illness, and may overlap with the fever stage. The convalescence stage ranges from 11 to 19 days after the onset of illness; during this time, clinical symptoms begin to resolve and laboratory parameters gradually return to normal.4)
In terms of disease progression, hemorrhagic fever with renal syndrome (HFRS), caused by the Hantaan virus (Bunyaviridae), is very similar to SFTS.1) The cardinal symptoms of HFRS are abrupt onset, fever, abdominal pain, oliguria, and thrombocytopenia.10) HFRS patients are believed to have infected renal endothelial cells, lead to disruption of endothelial permeability and dysfunction of the platelet inhibiting system. HFRS also triggers initiation of various signaling pathways that lead to release of pro-inflammatory chemokines and recruitment of immune cells at the site of inflammation. The inflammatory response triggers activation of the complement system and secretion of numerous pro-inflammatory cytokines that down-regulate renal endothelial function, causing proteinuria.8)
SFTS patients develop many of the same symptoms because the pathophysiology of SFTS appears similar to that of HFRS. A noteworthy difference is the high incidence of encephalitis in SFTS patients. A recent study reported that 19.1% of hospitalized SFTS patients had encephalitis, and that 44.7% of these patients died.2) We infer that SFTSV can infect the CNS, and thereby lead to a more serious or even fatal clinical outcome, probably through immunopathological damage.2)
This case reports a 70-year-old farmer with no document of tick bites, but who was probably infected while working outdoors. The patient's underlying hypertension and development of thrombocytopenia from SFTSV were responsible for development of acute SDH. Regarding the rapid progression of hematoma, rupture of cortical artery weakened by virus could be suspected.11) It is assumed that the mechanism of the arterial rupture is swinging of the brain inside the skull with minor trauma.67) Hypertension and thrombocytopenia could be significant contributing factors to this mechanism.12) Clinical analysis and PCR data provided by the National Research Institute of Health confirmed the diagnosis of SFTS. The pathophysiology of SFTS is still not entirely clear, but there is a suspected involvement of brain parenchyma. Further research is necessary to understand the pathophysiology and epidemiology of this disease.
Go to :
 XML Download
XML Download