

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Bilateral pedicle fractures in the spine are uncommon because they have a higher mechanical strength than the pars interarticularis, even in elderly patients.359) Furthermore, the pedicle has great intrinsic strength and a short moment arm, and can therefore resist greater cyclic shear forces.1) Spondylolysis, or fracture of the pars interarticularis, is the most common injury of the neural arch, and osteoporotic compression fracture is common in adjacent segments after instrumented fusion due to loss of motion at fused segments by altered biomechanics.79) However, bilateral pedicle stress fractures at adjacent cephalad levels after instrumented lumbar fusion are extremely rare because stress concentration on the proximal junction area is associated with severe junctional changes including adjacent compression fractures or stenosis. Here, we report a rare case of bilateral pedicle stress fractures, which were not detected before surgery at an adjacent upper level after instrumented lumbar fusion and not associated major trauma.
Go to : 
Case Report
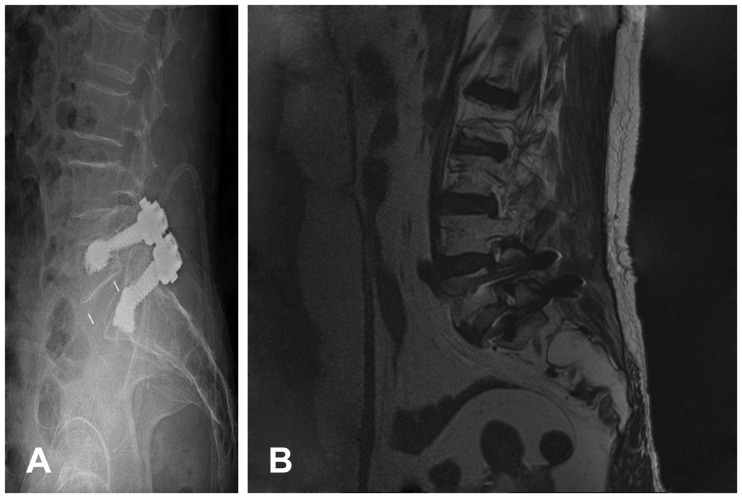
A 77-year-old woman was admitted to our institute with severe back and buttock pain. Four years previously, she underwent anterior lumbar interbody fusion (ALIF) with bone cement augmented screw fixation at the L5-S1 level under a diagnosis of foraminal stenosis. At that time, there were no pedicle fractures at the L4 level (Figure 1), and the lowest T-score by dual-energy X-ray absorptiometry (DXA) bone mineral densitometry was -3.8. The patient presented with only mild back discomfort after ALIF with screw fixation, but the back pain progressively worsened without any history of trauma for 2 months before re-admission. Ambulation was limited and the patient was re-admitted to our institute. A physical examination revealed neurologically intact status, but prominent tenderness was present in the low back area and back motion was reduced, especially in backward extension.
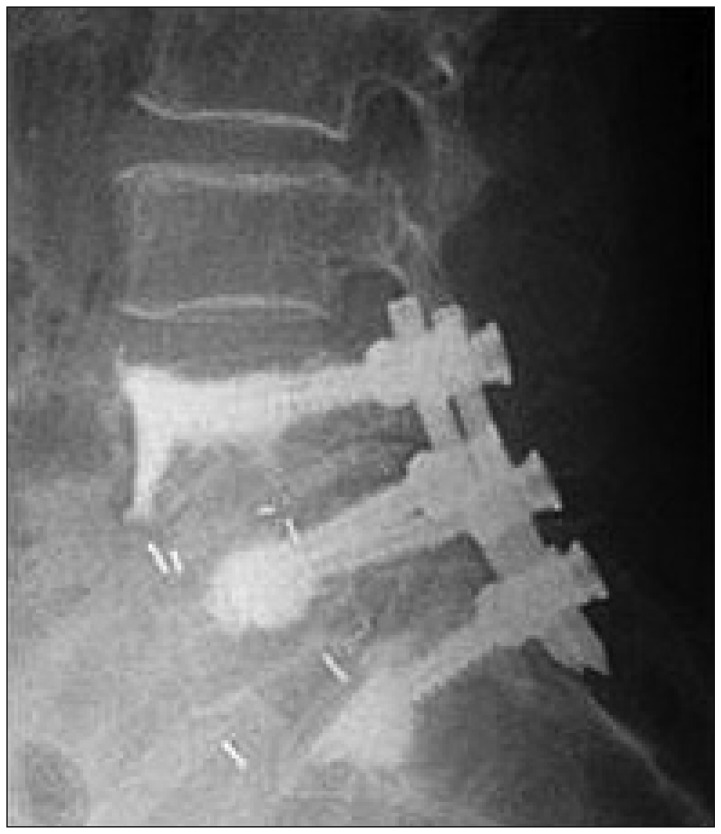
Plain radiographs showed marked irregularity of the L4 pedicle suggesting L4 pedicle fractures at both sides (Figure 2A), and magnetic resonance images and computed tomography scans revealed bilateral pedicle fractures through L4 accompanying foraminal stenosis at L4-5 level (Figure 2B-E). She was treated by posterior lumbar interbody fusion of L4-S1 with rigid screw (Figure 3). At her 8-month follow-up assessment, no residual lower back pain was evident and she had returned to normal activities.
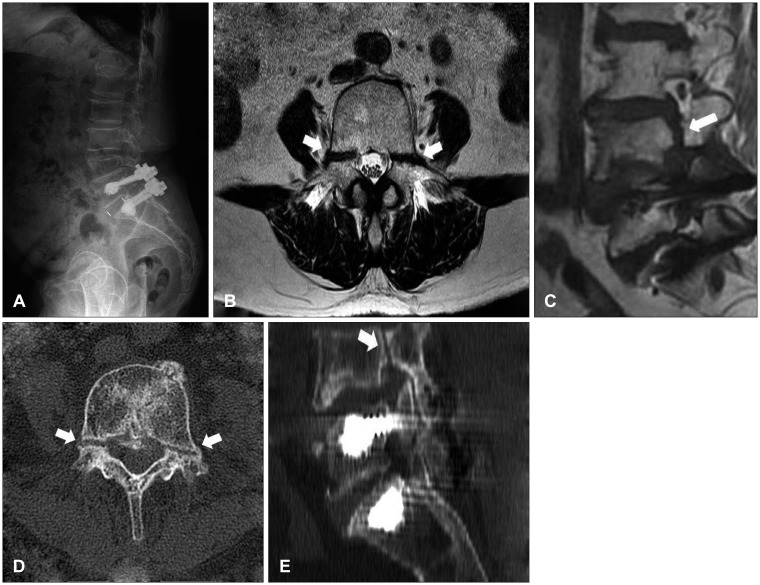 | FIGURE 2Radiological studies performed at 4 years after anterior lumbar interbody fusion with screw fixation. (A-C) Simple lateral radiograph and magnetic resonance images suggestive of pedicle fracture at the L4 level (arrows). (D,E) Computed tomography scans showing bilateral pedicle fractures without surrounding sclerosis (arrows).
|
Go to :
Discussion
Osteoporosis contributes to cephalad compression fractures
due to altered biomechanics in adjacent segments caused by junctional failures associated with loss of motion at fused segments.6) Fused lumbar segments may increase stress and motion at adjacent unfused segments and accelerate degeneration. However, adjacent fracture of bilateral pedicles after instrumented lumbar fusion is extremely rare and to our knowledge, no such case has been previously reported. Furthermore, bilateral pedicle fractures are rare and have only been reported on a few occasions.2458910) In these reported cases, most bilateral pedicle fractures were generally related to previous spine surgery or stress-related activities, and pedicle stress fractures after lumbar fusion surgery occurred at the most proximal or distal level of fusion.6) To our knowledge, three cases of bilateral pedicle stress fracture after lumbar fusion without screw removal have been reported,8910) and two of these cases occurred at the uppermost level of fusion.89) Tribus and Bradford10) described the case of a patient treated by posterior spinal fusion using segmental instrumentation from T3 to L4 who developed fractures of the lowest L4 pedicle. However, in this case, the adjacent upper level of the L4 pedicle was involved after instrumented L5-S1 fusion. Repetitive mechanical stress fractures in the posterior elements are usually located in the pars interarticularis or to a substantially lesser extent, in the pedicle. The pedicle has great intrinsic strength and a short moment arm from the vertebral body, and can therefore resist greater cyclic shear forces.4) As a result, the pedicle is an uncommon location of fracture at the posterior neural arch. Rather, fractures are more frequently observed in the isthmus, which corresponds to the weakest zone. Nevertheless, bilateral pedicle fractures at adjacent levels can occur due to surgically acquired disturbance of the neural arch. Adjacent pedicles associated with spinal fusion masses may experience abnormal repetitive shear forces and cantilever because of continued motion through intervertebral discs and the pars interarticularis.10) In our patient, the fractures appeared to be fresh, because no sclerotic change was evident at fracture margins in spite of the absence of a trauma history.6) We had performed bone cement augmented screw fixation at L5-S1 level. The overstiffness and enhanced strength may increase the risk of bilateral pedicle fractures of adjacent, non-augmented vertebrae, because of increased biomechanical stress. We fused the L4-5 segment to stabilize the pedicle fractures, and the solid stabilization may result in pain relief, and allowed our patient to return to normal activities.
Go to :
Conclusion
We report an uncommon case of bilateral pedicle fractures at the adjacent upper level of previous instrumented fusion without a history of evident trauma. Although it is rare, this report gives useful information to spine surgeons regarding the treatment and diagnosis of similar cases.
Go to :
 XML Download
XML Download