

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Each year, gunshot injuries constitute approximately 13% to 17% of all vertebra and spinal cord injuries.9) The severity of spinal damage due to gunshot injury depends on mechanical factors of the gun and biological factors. Damaging mechanism of this kind of injuries can be explained with velocity of the bullet and transfer of its kinetic energy to the tissue. Thus bullet dimensions and its velocity become the most important factors affecting magnitude of the tissue damage. On the other hand civilian guns have generally lower velocity and did not cause severe tissue damage.4)
Gunshot injuries to the spine at cervical level frequently cause spinal cord dysfunction and death as a result of respiratory distress followed by brainstem damage. In addition to neurological dysfunction, gunshot injuries to the cervical area may cause mechanical instability. Patients rarely gain their normal function after injuries of low velocity guns.12) Gunshot injuries do not have a clear treatment protocol. Incomplete neurological deficit, mechanical instability, cerebrospinal fluid fistula, risk of migration of the bullet or its fragments within the canal and bullet intoxication are generally accepted criteria for surgical operations.18) Irrespective of the indications of spinal surgery, additional organ injuries unfavorably affect survival in spinal gunshot injuries. In this case report, we shared the gunshot injury at C6-7 level which caused an incomplete isolated C7 root damage, treated surgically and resulted in a very good outcome which is not very common for this kind of injuries.
Case Report
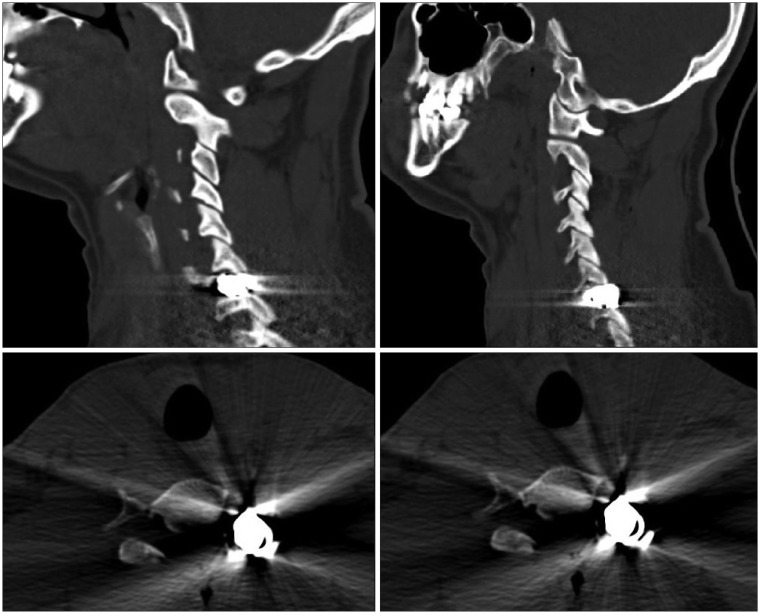
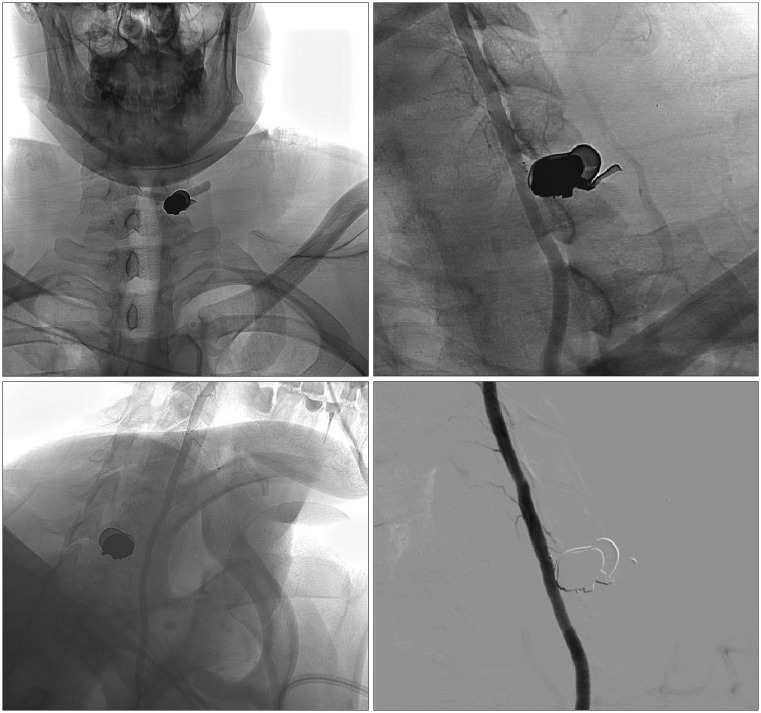
A 24-year-old male patient admitted to the emergency room with civilian gunshot injury. In physical examination, gunshot entrance wound was observed at left posterior cervical area. In neurological examination, severe pain in the left arm was detected; muscle strength was scaled 2/5 for extension of the left forearm and 3/5 for flexion of the left wrist. In cervical computerized tomography (CT), metallic hyperdensity on the left side facet joint level within range of C6-7 discs and bone fragment in C6-7 left paracentral area were detected (Figure 1). Because of close neighborhood of the metallic foreign body to left transvers foramen, digital subtraction angiography was realized to observe vascular damage in vertebral artery. Any finding related to laceration or dissection in vertebral artery was not detected (Figure 2).
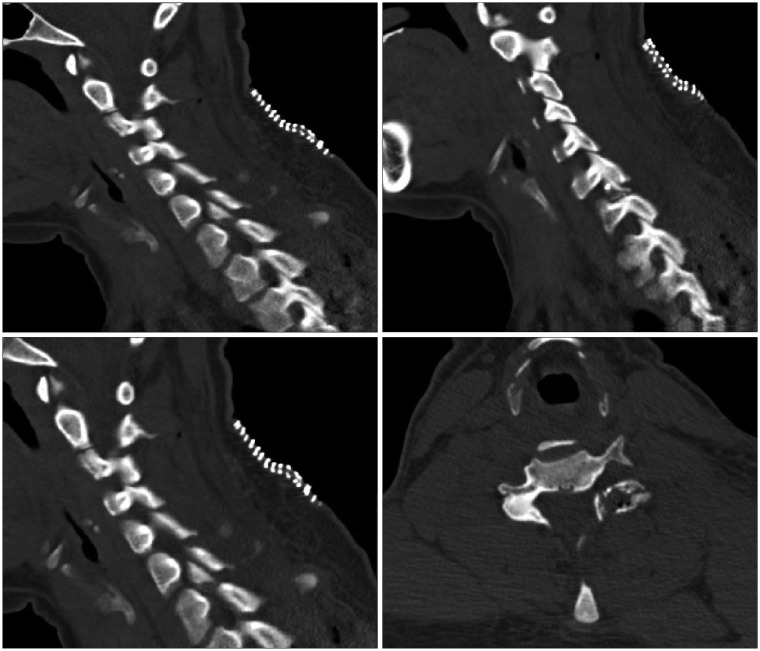
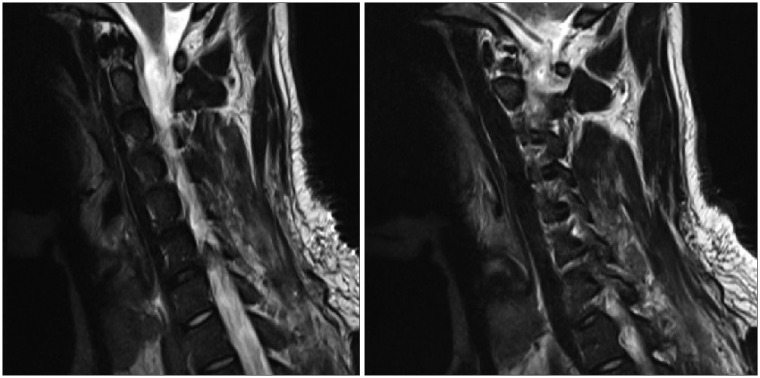
We decided for a surgical intervention provided that an incomplete neurological deficit was present and aimed to reduce the pain, the main current complaint. We performed emergent surgery on the patient. Metallic foreign body which was considered as bullet and compressing left C7 root on facet joint level of C6-7 disc and bone fragment in left paracentral area were removed with posterior approach. In postoperative early period neurological examination, muscle strength of the patient was detected 3/5 for extension of the left forearm and 4/5 for flexion of the left wrist. We checked with cervical CT that the metallic foreign body and the bone fragment were entirely removed (Figure 3). We observed changes secondary to operation in cervical magnetic resonance imaging at C6-7 corpus level. We did not detect any pathology compressing C7 root at C6-7 level (Figure 4).
A written consent for the publication of this report was obtained from the patient.
Discussion
Gunshot injuries to the spine constitute approximately 13% to 17% of all spinal cord injuries and are the third most common reason of spinal cord injuries after traffic accidents and falls from an elevation.5) Trauma intensity depends on localization. Spinal injuries are localized 48% to 64% on thoracic area, 19% to 37% on lumbar area and 10% to 29% on cervical area.71115) It is reported that the rate of injury to large vessels or to internal organs alongside with spinal injuries is 21% to 64%. Gunshot injuries to cervical area may also cause mechanical instability.310)
Treatment in gunshot wounds to the spine is still controversial. In military injuries, surgery is mostly suggested to prevent complications of large damages caused by high velocity guns. On the other hand in civilian injuries, damage is generally more limited due to lower velocity of the guns. Thus conservative approach with parenteral antibiotic treatment is suggested except for especially cauda/conus area wounds and progressive neurological deterioration.12310)
Indications for surgery with the main lines are progressive neurological deterioration; existence of compressing bone fragment, intervertebral disc or foreign body into the spinal canal; cerebrospinal fluid fistula; cauda/conus injuries; spinal instability; abscess formation and pain syndromes in late period. Consequently CT is highly important to determine integrity of these components. In case of instability, internal fixation should be realized. Henceforth patients can start early functional exercises.8) It has been reported by Robertson and Simpson17) that radicular pain in patients with penetrant caudal spinal injuries was recovered after decompressive laminectomy and removal of the fragment. Besides Waters and Adkins19) have reported that the pain was not relieved after removal of the bullet.
Vertebral artery injury is less observed than the other vascular components' injuries due to its profound location in cervical area and its well protection by bones, muscles and fascias.6) Vertebral artery injuries lead to ischemic neurological findings and high fatality rate. Symptoms are acute or slowly progressive unconsciousness, brainstem and cranial nerves findings, aphasia, dysphasia, facial paralysis, extraocular muscles paralysis, nausea, vomiting and dizziness.14) Angiography should be absolutely performed in di-agnosis of artery injuries to locate lesion, to define its type, to show existence of a vasospasm, obstruction, dissection, aneurysm and fistula; and also to observe vertebral artery of the opposite side.1620) Müller et al.13) have reported that vertebral artery damage was observed in 20% of the patients having transvers foramen fracture and in 31% of the patients having cervical subluxation/dislocation.
Conclusion
Although it was not a very difficult one, our decision for this case was surgical intervention due to an incomplete neurological deficit. Our case had decompressive surgery due to severe left arm pain and muscle weakness in the left forearm extension and in the left wrist flexion. We observed explicit relief in pain and recovery of left upper extremity weakness after removal of the bullet and the bone fragment. Surgical intervention is not often the chosen path for the treatment of gunshot wounds to the spine, nevertheless it might lead to very good outcomes in selected cases with incomplete neurological deficit.
 XML Download
XML Download