

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Posterior reversible encephalopathy syndrome (PRES) is a clinical and radiological syndrome, first described by Hinchey et al.5) in 1996. Most common clinical manifestations are headache, seizures, altered consciousness, transient motor deficits and loss of vision. The main finding in neuroimaging is posterior white matter edema, which is predominating in the occipital and parietal lobes and posterior fossa structures and which are potentially reversible, if prompt diagnosis and treatment would be performed.1) The disease has been more commonly described in adult population.11) The main causes of this condition include eclampsia, organ transplantation. Hypertensive crisis, immunosuppression, chemotherapeutic agents for lymphoma and leukemia, severe hypercalcemia, thrombocytopenic syndromes, Henoch-Schönlein purpura, vasculitis, and renal failure.513) Although there have been reports of PRES in children following chemotherapy and tumor lysis syndrome, the prevalence of PRES among children is not well established. We would like to report PRES occurred after head trauma surgery in pediatric patient without any underlying disease.
Go to : 
Case Report
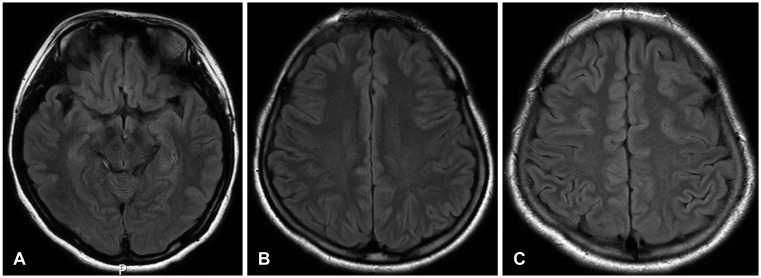
A 16-year-old girl without any medical history was referred to emergency room for drowsy consciousness due to motorcycle accident. Computed tomography (CT) scan showed comminuted fractures involving outer walls, inner walls and inter-sinus septum of frontal sinuses with depressed fractures, extending both orbital roofs and medial orbital walls with small contusion on frontal lobe (Figure 1A and B). Initial T2-weighted (T2W)/T2 fluid-attenuated inversion recovery (FLAIR) image presented no other significant lesion except small contusion in posterior temporal area (Figure 2A-C). There was no scalp laceration and cerebrospinal fluid (CSF) leakage. Medical treatment including antibiotics was performed for 14 days. During hospitalization, neurologic state was improved and vital sign including blood pressure (BP) was normal range. CSF leakage and meningitis sign were not observed. The patient was discharged without neurologic symptom and complication. After 14 days on discharge, the patient visited emergency room with rhinorrhea. Despite of bed rest and lumbar drainage for three days, CSF leakage was continued. Surgical treatment was planned. Dura repair, frontal sinus sealing, bony reconstruction and galeal reposition on skull base were performed. After surgery, CSF leakage was not observed and there were no surgical related complications. Three days after surgery, the patient presented several generalized tonic-clonic (GTC) type seizure. The vital sign and blood examination showed hypertension and mild elevated creatinine (systolic BP [SBP], 140–160 mmHg; creatinine, 2.3 mg/dL). Followed by a retrospective review, BP was shown gradually increasing tendency after surgery. Magnetic resonance imaging (MRI) showed high signal in T2W/T2 FLAIR image, suggesting cerebral edema involving the subcortical white matter of bilateral frontal, temporal, parietal, and occipital lobes, with few areas of cortical involvement (Figure 3C). Under provisional diagnosis of PRES based on radiologic findings and clinical symptoms, we started antiepileptic and antihypertensive agents. The patient improved clinically and discharged with no neurologic deficit. After 3 months on follow-up, MRI showed that previous edematous lesions were completely disappeared (Figure 4A-C). Antiepileptic and antihypertensive agents were stopped and BP has been well maintained in normal range.
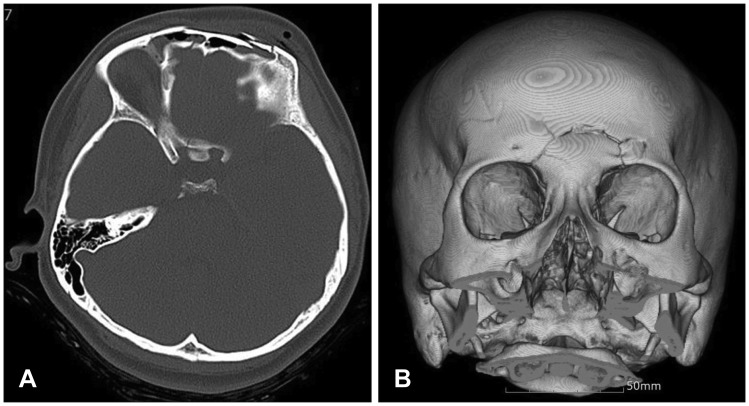 | FIGURE 1(A, B) Computed tomography scan showed comminuted fractures involving outer, inner walls & inter-sinus septum of frontal sinuses with depressed fractures, fractures extending both orbital roofs & medial orbital walls and small contusion on frontal lobe with drowsy consciousness.
|
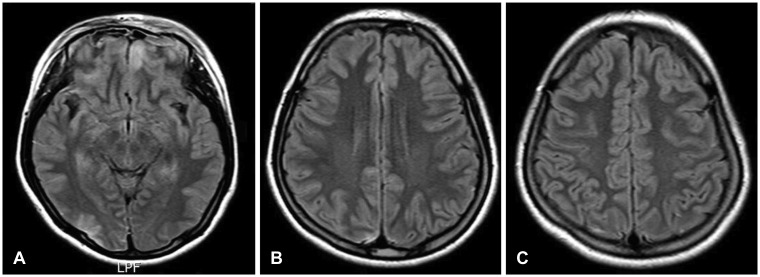 | FIGURE 2Initial brain magnetic resonance imaging after head injury. (A–C) Initial T2-weighted/T2 fluid-attenuated inversion recovery image presented no other significant lesion except small contusion in posterior temporal area.
|
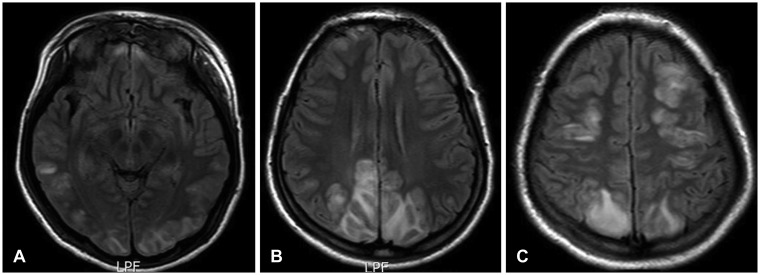 | FIGURE 3Brain magnetic resonance imaging (MRI) 3 days after the surgery with generalized seizures. (A–C) MRI showed high signal in T2-weighted/T2 fluid-attenuated inversion recovery image, suggesting cerebral edema, involving the subcortical white matter of bilateral frontal, temporal, parietal, and occipital lobes, with few areas of cortical involvement.
|
Go to :
Discussion
The most common clinical manifestations of PRES are headache, nausea and vomiting, altered mental status, decreased alertness, seizures, cortical blindness, and transient motor deficits. In the patients with PRES, seizures are common at the onset of neurologic symptoms but can also develop later. The seizures are usually GTC type and/or multiple. Temporary restlessness and agitation may alternate with lethargy. Stupor and coma may develop. The patients are often confused and there may be some abnormalities of vision such as hemianopia, blurred vision, and cortical blindness.1214) Many predisposing factors have been proposed including hypertensive crisis, immunosuppressive drugs, eclampsia, and renal dysfunction. But, there were some differences in the etiological factors between the children and the adults, as in the clinical features. Although significant elevation of the BP may not always be demonstrated, hypertension has often been emphasized as a common feature of PRES-associated conditions.1) The pathophysiology underlying PRES is yet thoroughly demonstrated. Two theories are considered in the pathophysiology of PRES, the first being sudden increase in BP causing vasospasm and the other being failure of autoregulatory mechanism.13) With sudden elevation in systolic BP, the autoregulatory capacity of brain vasculature is exceeded which results in a region of vasodilatation and vasoconstriction, especially in the arterial boundary zone. This causes breakdown of the blood-brain barrier with subsequent transudation of fluid along with hemorrhage.12) The preferential involvement of the posterior circulation has been postulated as being due to the sympathetic innervation protecting the brain from sudden increase in BP being relatively less in the arterioles supplied by the vertebrobasilar system than in the anterior circulation.7) Considering the rare frequency of arteriosclerosis and good plasticity of vessel walls in children, the vulnerability of vessel walls to hypertension might be decreased in childhood.8) But noteworthy, children sometimes may be regarded to be more vulnerable to cerebrovascular dysfunction than adults under systemic hypertension because they have a narrower range of autoregulation in cerebral blood flow.3) Thus, it is possible that pediatric patients are more susceptible to PRES, and if so, this could be underrecognized in the literature.10) Postoperative hypertension is a common complication resulting from surgical intervention and occurs not only in those with pre-existing uncontrolled hypertension, but also in those who were normotensive or well controlled with medication. Given these characteristics, in our case, we thought PRES might be occurred due to post-operative transient hypertension. Some case reports show that CSF leak and intracranial hypotension can cause PRES.24) In this case, there is no evidence of CSF leak in the first stage of PRES, therefore it is reasonable that postoperative hypertension cause PRES. The symptoms and lesions of PRES may resolve completely if the diagnosis and treatment is prompt, as was seen in our patient. However, failure to diagnose may lead to irreversible infarction and death.69) Recurrence of PRES is rare and may be associated with infections and rapid rise in BP.13) The diagnosis may be overlooked, especially in children, unless a high index of suspicion and precise clinical history is maintained.
Go to :
Conclusion
The PRES has been more commonly reported in adult population, especially with underlying disease. But because the pediatric patients may be more vulnerable to cerebrovascular dysfunction than adults under systemic medical problems such as transient hypertension, if the children had no previous underlying disease, it is important that PRES should be kept as a possibility in children presenting with encephalopathy and seizures along with radiologic findings. Under surgery or treatment procedure in pediatric patients, more attention about vital sign and/or general function should be paid in intra and postoperative periods.
Go to :
 XML Download
XML Download