

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Decompressive craniectomy (DC) is the therapy of choice for life-threatening space-occupying intracranial pathologies, such as intracerebral bleeding, and traumatic or ischemic brain swelling.182327) After the resolution of cerebral swelling and the consolidation of the clinical state, cranioplasty (CP) is performed, not only as a cosmetic and protective measure, but because of curative effects on cerebral hemodynamics and metabolism.82433) Various materials have been used for CP, including autologous bone, polymethyl methacrylate (PMMA), ceramics, hydroxyapatite, polyetheretherketone, carbon-fiber-reinforced polymer and titanium.1) There is still no consensus on the ideal materials. Two of most commonly used materials are autologous bone flaps and PMMA.3) Autologous bone flaps are inexpensive, perfect matches to the bone defects, and do not induce tissue reactions; however, there are some reports of increased risks of infection and bone resorption.9) PMMA cost-effective, stronger than the adjacent bone, can be shaped as required, and is associated with minimal inflammatory reaction; however, high rates of infection have been reported.6)
The objective of the current study was to compare the rates of complications, and the possible risk factors for complications, in patients who underwent CP using sterilized autologous bone flap or PMMA. We investigated the two most common complications following CP: bone flap resorption (BFR) and surgical site infection (SSI).
Go to : 
Materials and Methods
Data collection
We retrospectively analyzed data from 127 patients who underwent CP after DC between January 2004 and December 2013. All the participants were indicated for unilateral CP and totally 127 cases were reviewed. The medical records, plain skull radiographs, and brain computed tomography (CT) of the patients were reviewed. The patients were divided into two groups according to the material used. Group I included 97 patients (76.4%) who underwent CP using a PMMA prosthesis, whereas Group II included, 30 patients (23.6%) who underwent CP using sterilized autologous bone flap. All patients were followed for at least 12 months, and the mean follow-up period was 15 months (from CP to last outpatient department follow-up appointment). Follow up included clinical and CT examinations, and appointments were scheduled for 6 weeks, 3 months, 6 months, 12 months, and then every 12 months after CP. For patients with a suspected or obvious complication, this follow-up regimen was adjusted depending on clinical and radiological findings. Perioperative and postoperative complications were recorded. Data collected included sex, age, initial diagnosis (reason for DC), time interval between DC and CP, operation time, method of bone flap fixation (miniplates or nylon sutures), size of the bone flap, and existence of a preoperative ventriculo-peritoneal (V-P) shunt. The size of the bone flap was classified as small (<75 cm2), medium (75-125 cm2), or large (>125 cm2), according to the formula: π/4×long axis×short axis. Patient data were analyzed in order to identify risk factors for BFR and SSI.
Sterilization and preservation of autologous bone flap
The bone flap removed during DC was cleansed of any remaining soft tissue and dried at 110℃ to 120℃ for 24 to 48 hours in Olympic Sterile Driers (Natus Incorporated, Middleton, WI, USA). The bone flap was then, sterilized at 70℃ for 75 minutes with a Sterrad® NXTM Sterilization System (Advanced Sterilization Products, Irvine, CA, USA) that uses hydrogen peroxide and low-temperature gas plasma to sterilize materials without leaving toxic residues. After this process, the bone flap was aseptically sealed in a double sterilization bag with a patient-identification label, and stored in a refrigerator at 8℃. Twelve hours before planned CP, the bone flap was sterilized again at 70℃ for 75 minutes.
PMMA prosthesis
The powder polymer was added to the liquid monomer (catalyst) to be totally dissolved by continuous stirring for about 15 minutes. After mixing, the mixture reached mouldable viscosity and was poured into the cranial defect. The dura and brain were protected from the heat produced from the PMMA polymerization process by placement of moist gauze between the dura and the hardening prosthesis. The PMMA prosthesis was shaped to achieve a smooth surface conforming to the normal contours of the skull.
CP procedure
The skin was cut along the previous DC incision and separated from the cranium, dura, and the underlying temporalis muscle. The temporalis muscle was then carefully dissected as a separate layer from the dura, avoiding any leakage of cerebrospinal fluid. After trephination of multiple holes to enable suturing of the flap, suturing of the flap, the flap (either autologous bone flap or PMMA) was fixed in it was fixed in position, as close to the edge of the bone defect as possible, using either miniplates or nylon sutures. All patients received prophylactic antibiotics and had a subgaleal drain for five days after CP.
Evaluation of BFR
We categorized BFR into two different types according to the features observed using CT with a window width level of 2500/500 HU. Type 1 was defined as BFR along the edge of the bone flap at the time of CP. Type 2 was defined as a complete lysis or major partial resorption of the bone flap, resulting in the loss of brain protection, and, occurring at least a year after CP (Figure 1). In our institution, Type 2 BFR was an indication for surgical resection of necrotic bone and secondary CP using PMMA.
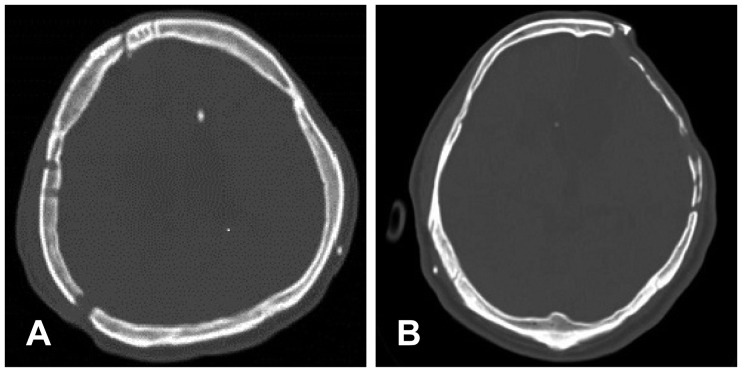 | FIGURE 1The different types of bone flap resorption (BFR) according to our classification: (A) Type 1 BFR showing bone resorption along the edge of the bone flap at the time of cranioplasty (CP), and (B) Type 2 BFR, showing a complete lysis and partial bone resorption of the bone flap 18 months after CP.
|
SSI
CP-related SSI was defined as an infection of the flap transplanted during CP, requiring surgical removal of the infected flap. Focal inflammatory signs, such as local swelling, redness, and/or low-grade fever that healed without the removal of the transplanted flap were excluded
Statistical analyses
Data were analyzed using R language version 3.01 (R Foundation for Statistical Computing, Vienna, Austria) and p-values <0.05 were considered statistically significant. Continuous variables are summarized as mean±standard deviation and categorical variables are summarized as N (%). Statistical significance for comparisons between two groups was tested using the 2-sample t-test or Wilcoxon rank sum test for continuous variables. Categorical variables were compared using Pearson's chi-square test or Fisher's exact test.
Go to :
Results
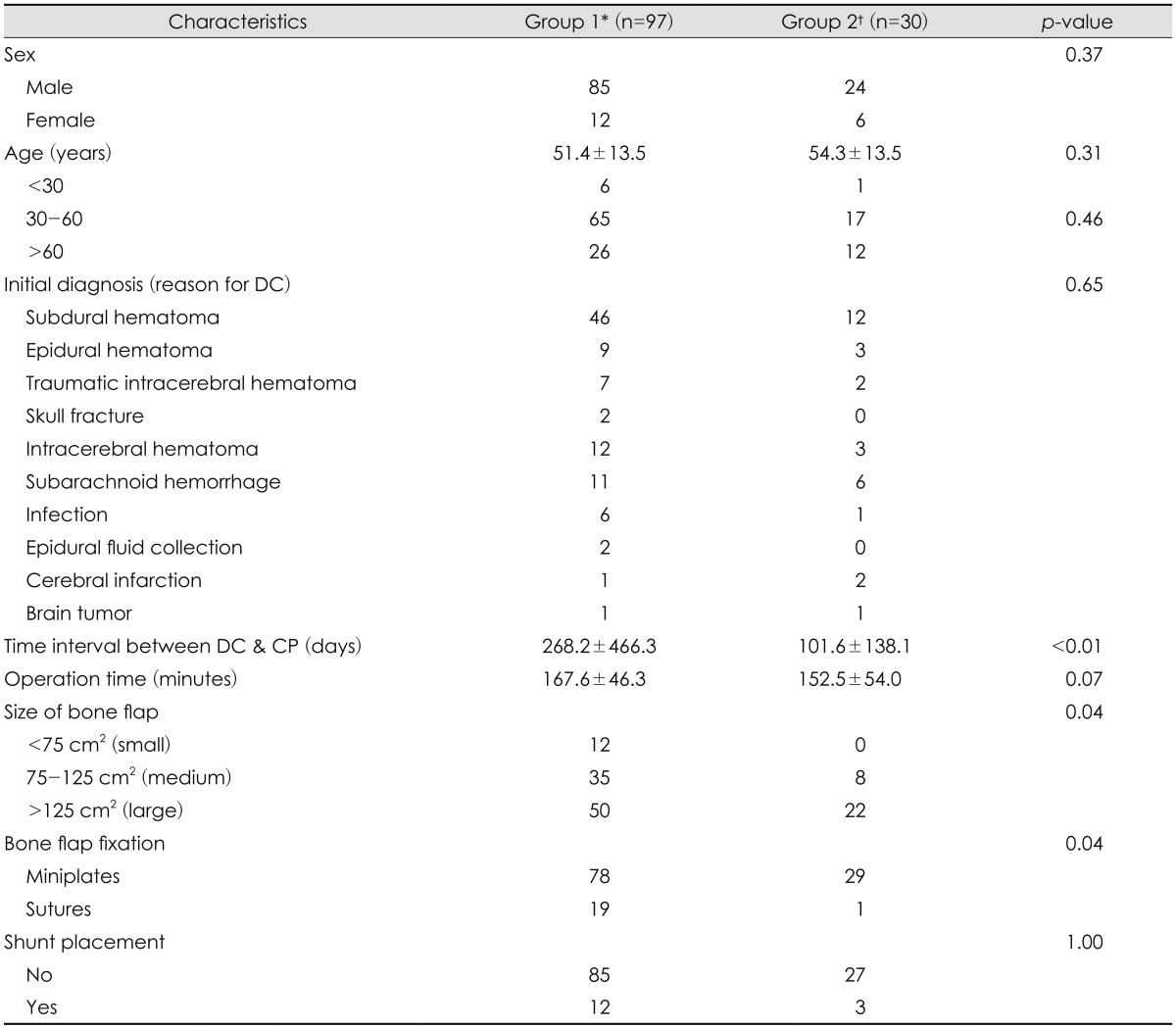
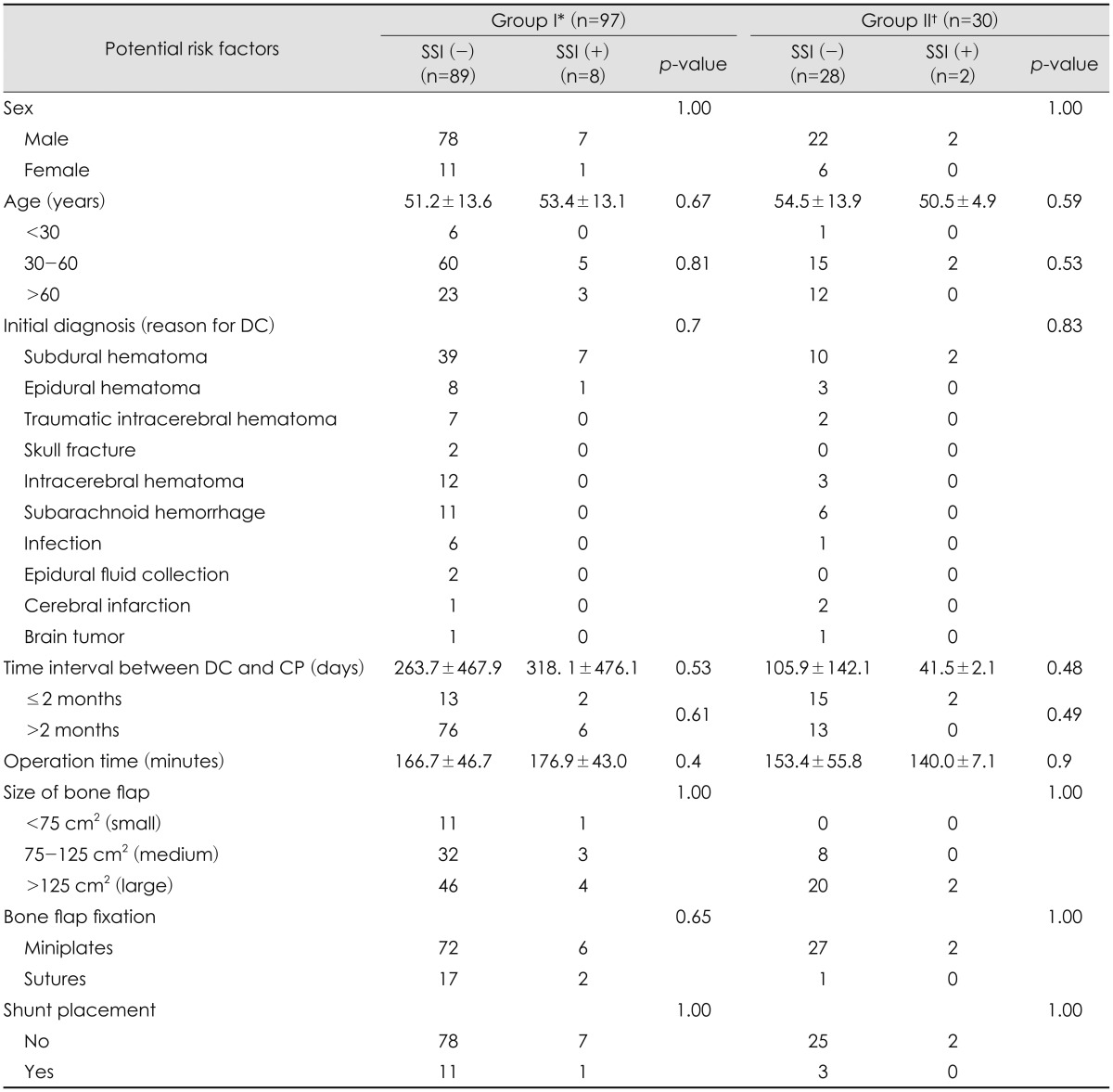
The clinical characteristics and perioperative data for patients in Group I (who received prosthetic PMMA) and Group II (who received sterilized autologous bone) are summarized in Table 1.
Sex and age
In Group I, there were 85 male and 12 female patients, with a mean age of 51.4±13.5 years. In Group II, there were 24 male and 6 female patients, with a mean age of 54.3±13.5 years. There were no statistically significant differences between the two groups in relation to sex (p=0.37) or age (p=0.31).
Initial diagnosis (reason for DC)
The initial diagnoses were divided into ten general categories; 1) subdural hematoma (SDH), 2) epidural hematoma (EDH), 3) traumatic intracerebral hematoma, 4) skull fractures, 5) intracerebral hematoma (ICH), 6) subarachnoid hemorrhage (SAH) due to ruptured aneurysm, 7) infection, such as cerebral abscess or, subdural empyema, 8) epidural fluid collection (EFC), 9) cerebral infarction, and; 10) brain tumor. There was no statistically significant difference in initial diagnosis between Group I and Group II patients (p=0.65).
Time interval between DC and CP
For Group I patients, the time interval between DC and CP was 268.2±466.3 days, and for Group II patients the time interval between DC and CP was 101.6±138.1 days (p<0.01).
Operation time
The mean operative time for Group I and Group II patients was 167.6±46.3 minutes and, 152.5±54.0 minutes, respectively. There was no statistically significant difference between the two groups (p=0.07).
Size of bone flap
In the Group I patients, 12 flaps (12.4%) were small, 35 flaps (36.1%) were medium-sized, and 50 flaps (51.5%) were large. In Group II patients, 8 flaps (26.7%) were medium-sized and 22 flaps (73.3%) were large, and there were no small flaps. The difference between the size of the bone flap in Group I and Group II patients was statistically significant (p=0.04).
Bone flap fixation
In Group I patients, 78 flaps (80.4%) were fixed with miniplates, and 19 flaps (19.6%) were fixed using nylon sutures. In Group II patients, 29 flaps (96.7%) were fixed with miniplates, and only one flap (3.3%) was fixed using nylon sutures. The difference between the method of fixation of the bone flap in Group I and Group II patients was statistically significant (p=0.04).
Preoperative V-P shunt
In Group I patients, a V-P shunt was present in 12 patients, whereas in Group II patients, a V-P shunt was present in 3 patients. There was no statistically significant difference between Group I and Group II patients (p=1.00).
Assessment of complications
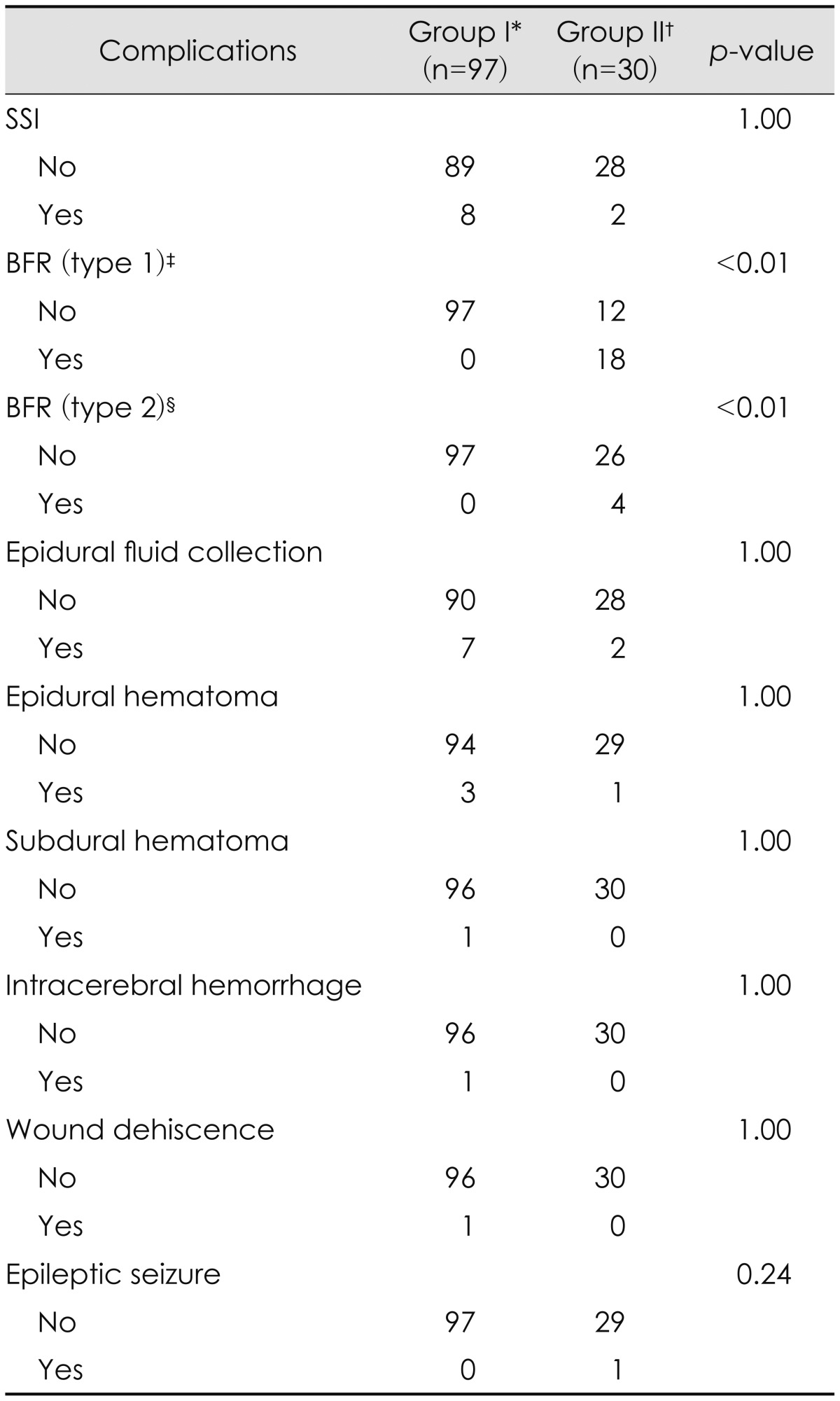
Complications in each group are shown in Table 2. In Group I patients, postoperative complications included SSI in 8 patients (8.2%), EFC in 7 patients (7.2%), EDH in 3 patients (3.1%), SDH in 1 patient (1.0%), ICH in 1 patient (1.0%), and wound dehiscence in 1 patient (1.0%). In Group II patients, postoperative complications included, SSI in 2 patients (6.7%), EFC in 2 patients (6.7%), and EDH in 1 patient (3.3%). There were no statistically significant differences between Group I and Group II patients regard to the rate of complications, with exception of BFR. In Group I, no incidences of BFR were recorded. In Group II patients, however, Type 1 BFR occurred in 18 patients (60.0%) and Type 2 BFR occurred in 4 patients (13.3%). The difference between Group I and Group II patients with regard to BFR is statistically significant (p<0.01).
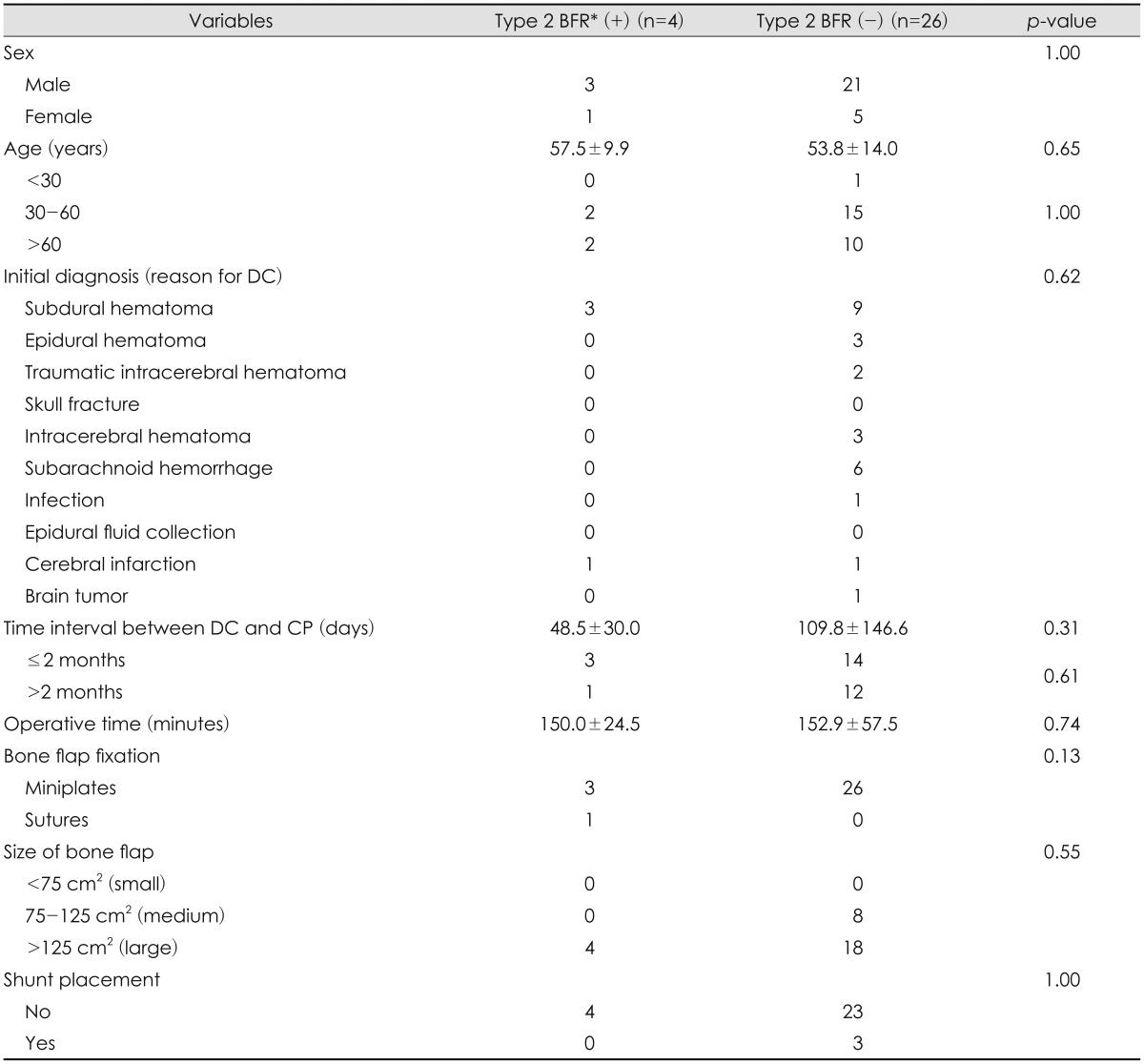
Risk factors for Type 2 BFR
The risk factors for Type 2 BFR, which only occurred in Group II patients, are listed in Table 3. To identify the risk factors predisposing to Type 2 BFR, patient data (sex, age, initial diagnosis, time interval between DC and CP, operative time, size of bone flap, and presence of a V-P shunt) were investigated, but, no statistically significant risk factor was found.
Assessment of risk factors for SSI
The occurrence of infection and related risk factors are summarized in Table 4. In Group I patients, SSI occurred in 8 patients (8.2%), whereas in Group II, SSI occurred 2 patients (6.7%) (p=1.00). Variables, including sex, age, initial diagnosis, time between DC and CP, operation time, size of bone flap, and presence of a V-P shunt, were analyzed to identify the risk factors for SSI, but, no statistically significant risk factors for SSI were identified.
Go to :
Discussion
CP is a commonly performed operation in the field of neurosurgery, however, it has a higher complication rate than other types of elective craniotomy.20) According to recent studies, the rates of complications after CP ranged from 16.4% to 34%, and varied according to the type of procedure and materials used.2357929) Two of most commonly used materials are autologous bone flaps and PMMA.3)
Although many clinicians have investigated what methods of autologous bone flap sterilization and preservation is better over several decades, there is currently no standard guideline for the sterilization and preservation of skull bone flaps for CP. The most commonly used techniques for preserving the autologous bone flaps involve cryopreservation and subcutaneous implantation into the abdominal pocket.20)
BFR is one of the known long-term complications of CP following DC. It has been reported in 7.2% to 50% of cases. Hallfeldt et al.11) reported that sterilization of bone by autoclaving had a negative effect on osteoinductive properties, resulting in poor new bone formation. Additionally, Osawa et al.21) demonstrated that frozen bone showed similar microscopic features to normal fresh bone, whereas osteocytes were destroyed in autoclaved bone. However, Mracek et al.20) demonstrated that preservation technique by boiling, autoclaving and storing of a bone flap in a refrigerator at 8℃ could be a suitable alternative method and relatively successful outcome for CP have been obtained for 40 years using this technique. Kim et al.14) recently reported a preservation technique that involved drying the autologous bone flap at 110℃ to 120℃ for 24 to 48 hours, sterilization at 70℃ for 75 minutes, storing the flap aseptically at room temperature, and then sterilizing at 70℃ for 75 minutes 1 to 2 days before the planned CP. They reported that BFR (equal to Type 2 BFR in current study) occurred as a long-term complication in 9 of 162 patients (5.6%). In our study, the method of sterilization is similar to that of Kim et al.14), but the flap was stored in a refrigerator at 8℃ and sterilization was performed 12 hours before the planned CP. In our study, Type 1 BFR (resorption along the edge of the bone flap at the time of CP) occurred in 18 patients (60.0%) undergoing CP using sterilized autologous bone flap. Type 2 BFR (complete lysis or major partial resorption of the bone flap with loss of the bony protection of the brain, which occurred at least one year after CP) occurred in 4 patients (13.3%) undergoing CP using sterilized autologous bone flap. According to Kim et al.14), BFR occurred significantly more often in patients who underwent DC due to TBI than those due to any other primary diagnoses (8.5% vs. 1.8%, respectively). Since patients with TBI comprised a larger portion of the sample in current study than that of Kim et al., our study resulted in a relatively higher rate of BFR.
The other aim of our study was to identify the risk factors for Type 2 BFR. Several authors have reported on the risk factors for developing BFR following CP with autologous bone. Schwarz et al.28) found that younger than 30 years, the presence of a V-P shunt, and bone flap fragmentation were risk factors for BFR. In addition, Martin et al.16) reported that the rate of BFR as 81.8% among 27 patients under 18-years of age who underwent CP with autologous bone after DC, following surgical revision in 54.4 %. In the current study, age was categorized into three subgroups22); <30 years of age, 30 to 60 years of age, and >60 years of age, but we found no significant relationship between incidence of BFR and age (p=0.65) (Table 3). We observed one 16-year-old female patient, who underwent DC to alleviate severe brain swelling resulting from traumatic brain injury (TBI). Three months after DC, she received CP using sterilized autologous bone. Progressive BFR was observed during serial follow up for 18 months after CP. Because of severe destruction of the contour of skull, the resorbed bone flap was removed and secondary CP, using PMMA, was performed. No BFR, SSI or other complications were reported during the follow-up period (Figure 2). As previously reported by Bowers et al.4), the presence of a V-P shunt tends to result in higher rates of BFR, both in children and in adults. Bowers hypothesized that, in children, skull growth depends upon regular brain development that results in an increase in brain volume. Shunt placement reduces fluctuations in intracerebral pressure and may, therefore, negatively influence skull growth and, contribute to BFR. They found that the placement of a V-P shunt also increased risk of BFR in adults. In the current study, however, we found that the implantation of a V-P shunt before CP was not significantly associated with BFR (p=1.0) (Table 3).
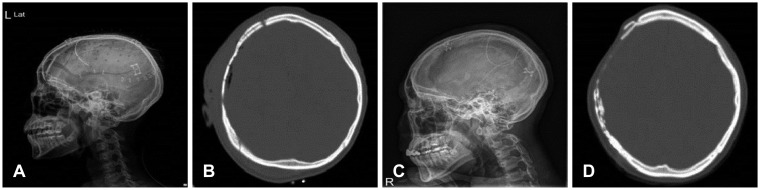 | FIGURE 2(A) Simple skull lateral X-ray and (B) brain computerized tomography (CT) scan show bone flap resorption (BFR) along the edge of the bone flap in the immediate postoperative period. Eighteen months after cranioplasty, (C) simple skull lateral X-ray and (D) brain CT scan show complete lysis of the bone flap.
|
Schuss et al.26) reported that the incidence of BFR was more frequent in patients with multiple fractures or fragments in the reinserted bone flap than in patients without multiple fractures or fragments (17.2% vs. 2.2%, respectively). In our institution, PMMA was used in patients with multiple skull fractures, and none of these patients developed BFR.
Grant et al.10) found a correlation between higher rates of BFR and size of skull defect; bone flaps larger than 75 cm2 had higher resorption rates than smaller bone flaps. However, this was not the case in the current study (p=0.95). Some studies investigated the relationship between BFR and TBI. In the current study, however, initial diagnosis did not predict the rate of BFR.
Mracek et al.20) suggested that firm fixation of the bone flap seem to be important factors in the risk of BFR. They found the fixation of the bone flap by sutures (which is less rigid than when fixing the flap using miniplates) resulted in a trend towards a higher rate of BFR, but, it was not statistically significant in the current study (p=0.16).
Schuss et al.26) found that 60% of BFR occurred within 1 year of follow-up and that no resorption was observed among patients followed for more than 5 years. However, in a study by Grant et al.10) of patients younger than 19 years, BFR occurred a mean 13.3 months (range, 2-76 months) after CP. In the current study, the mean follow-up period for all patients was 15 months (range, 12-127 months). The time interval between DC and CP did not predict the development of BFR in the current study (p=0.31). Patients were stratified into two groups according to the time interval between DC and CP (early, ≤2 months, and late, >2 months).25) There was no significant difference of BFR in two groups (p=0.61) (Table 3).
In adults, PMMA is still considered to be the best allograft material for CP.6) In our institution, PMMA was used in patients who did not have autologous bone available (either because they underwent operations in other hospitals or their operation history was not clear) or who needed re-operation due to complications such as BFR, SSI and EFC after using autologous bone. In addition, when patients had multiple skull fractures or bony fragmentation during DC, PMMA was the material used for CP.
Another aim of our study was to identify the risk factors for CP-related SSI, especially the association between the CP material used and potential risk factors. In previous studies, the reported rate of SSI varies between 0% and 25.9% with an average of 7.7%.20) In our study, the overall infection rate was 7.9%, which is comparable with other studied. Some previous reports demonstrated an increased rate of SSI associated with PMMA,1719) although a recently published report did not support this finding.3) In the current study, the group receiving PMMA had a SSI rate of 8.2% (8/97), whereas the group receiving sterilized autologous bone flap group had a SSI rate of 6.7% (2/30). There was no statistically significant difference between the two groups (p=1.00) (Table 2).
Previous studies reported that a longer time interval between DC and CP increased the risk of SSI.12) Recently, however, Sundseth et al.30) found no statistically significant relationship between the time interval from DC to CP and the risk for SSI. In the current study, the time interval between DC and CP was longer in patients receiving PMMA than in patients receiving autologous bone, but, there was no association with risk of SSI for either of the two groups of patients.
According to Tokoro et al.31) and Mracek et al.20), longer operation time was the significant risk factor for SSI. However, there is no significant association of SSI with longer operation time for either of the groups in the current study. This corresponds with two recently published studies by Kim et al.13) and Lee et al.15).
The presence of a V-P shunt has also been correlated to an increased rate of SSI in a previous study,25) but we did not find an increase in the rate of SSI between patients who had a V-P shunt in place and those who did not. Walcott et al.32) found that patients with stroke had a higher risk of SSI after CP than trauma patients. In the current study, however, there was no statistically significant association between the initial diagnosis and SSI following CP.
Our study has several limitations. The data analysis was retrospective, so limitations include all the anticipated deficiencies of a retrospective analysis, including the loss of patient information and poor follow-up. Due to the small sample size, it was difficult to identify significant risk factors conclusively. Analyzing the risk factors for BFR and SSI following CP is important, therefore, further clinical studies including much larger numbers of patients are needed
Go to :
Conclusion
In the current study, CP using sterilized autologous bone flap showed a significant increase in rate of BFR. PMMA, however, is a safe alloplastic material for CP, as it resulted in no BFR and a relatively low infection rate. PMMA is the choice of graft material for CP, for patients who need re-operation due to complications such as BFR and SSI. We have found no possible risk factors for BFR and SSI. Therefore, a large number of patients is needed to identify which factors affect BFR and SSI following CP.
Go to :
 XML Download
XML Download