

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Chronic subdural hematoma (CSDH) is a neurological disease of the elderly, with a mortality rate of 0.5% to 4%.615) Known risk factors are mild head injury, advanced age, alcohol abuse, coagulopathies, and therapeutic anticoagulation.614) CSDH is commonly managed by single or double burr hole trephination with or without closed system drainage and twist drill craniotomy.3) However, some severe complications, such as intracerebral hemorrhage (ICH), acute subdural hematoma (SDH), and subarachnoid hemorrhage (SAH) may impair the postoperative course and increase morbidity and mortality.8) We present a patient with SAH with multiple small ICHs in both cerebral hemispheres following evacuation of a bilateral CSDH.
Go to : 
Case Report
A 77-year-old man was admitted with severe disturbance of speech and progressive weakness on the right side. He had suffered minor head trauma one month prior. There was no medical history except diabetes mellitus, and clotting profiles were normal. A brain computed tomographic (CT) scan revealed that a bilateral CSDH of which there were more lots of quantities to the left which displayed the midline shift and compressed a ventricle with the right side (Figure 1A). Diffusion-weighted images (DWI) and gradient echo (GRE) images presented no acute ischemic and hemorrhagic lesions in the intracerebral region (Figure 1B and C). The patient got the operation which inserted the catheters through the burr holes made in the both sides of parietal area under the local anesthesia. The subdural spaces were irrigated with warm physiological saline and closed system drainages were inserted through each burr hole. He was stable during the operation and his blood pressure was well controlled. However, immediately after the procedure, he developed left side weakness grade III and confused mentality. A repeat brain CT scan showed a SAH at the bilateral frontoparietal cortex with multiple punctate ICHs bilaterally (Figure 2). CT angiography did not reveal cerebral aneurysms and vascular malformations. He admitted to intensive care unit for close observation and conservative treatment such as hemostatic agents and mannitol for controlling brain edema was adopted. After three days, right side motor weakness was completely recovered but, left side weakness was grade IV. After six days, his mentality became clear. He received a rehabilitation treatment repeatedly. After one month, the patient fully recovered and was discharged.
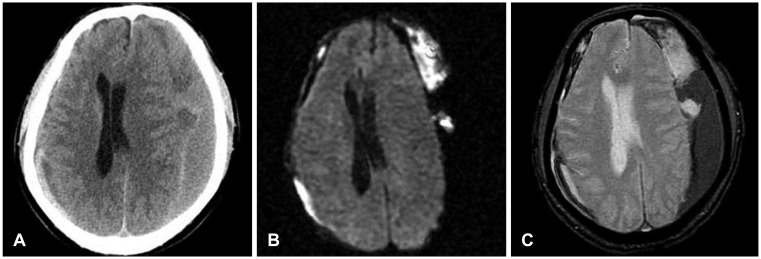 | FIGURE 1(A) Preoperative computed tomographic scan showing bilateral chronic subdural hematomas with a severe shift of the midline structures. (B) Diffusion-weighted image showing an absence of acute ischemic lesions. (C) Gradient-echo image showing no evidence of cortical and intraparenchymal hemorrhagic contusions.
|

Go to :
Discussion
CSDH is a liquefied old clot of blood between the surface of the brain and the dura mater. These liquefied clots most often occur in the elderly who have severe brain atrophy with minor head trauma which can cause tearing of fragile small blood vessels on the brain surface, resulting in a slow accumulation of blood clots over several days to weeks.1) Burr hole evacuation of the hematomas with or without closed system drainage is the safest and most effective neurosurgical procedure for treating symptomatic CSDH.516) Although the prognosis after surgery is good, critical and devastating postoperative complications may occur, including acute SDH, CSDH recurrence, seizure, and infection.9101415) However, several neurosurgical managements to evacuate CSDH may rarely be complicated by cortical hyperemia beneath the hematoma, SAH, and ICH in the ipsilateral or remote side of a SDH, diffuse cortical, and deep intracerebral.8914)
ICH at the brainstem after surgical decompression of a CSDH was reported first by Mckissock et al.7) in 1960. Mori and Maeda10) reported in their series of 500 CSDH that postoperative putaminal ICH developed at a rate of 0.2%. Modesti et al.9) reported in a detailed clinical review that incidence of ICH among 140 surgically treated patients with chronic extracerebral fluid collections was 5%. They noticed that there was no radiologic evidence of cerebral contusion or hematoma and no blood coagulation abnormalities in the clotting profiles, including prothrombin time, partial thromboplastin time, and platelet count in their series at the time of initial evaluation as they were in our patient.
Many pathologic conditions can contribute to development of ICH or SAH after evacuation of a CSDH. The most likely mechanism responsible for these problems is the combination of impaired vascular autoregulation due to long-term brain compression by CSDH and a rapid decrease of intracranial pressure after the drainage of the hematoma leading to hyperperfusion and cortical hyperemia, resulting in the rupture of a weak subarachnoid vessel.13) Moreover, focal cerebral edema beneath the compressed surface of the brain due to impeded venous drainage can reduce cerebral blood flow in the affected hemisphere. Chronic dilatation of small arterial vessels and loss of carbon dioxide reactivity in the ischemic hemisphere could also contribute to the pathogenesis.9) However, Dinc et al.2) reported that hemorrhage into undetected areas of contusion, damage to cerebral vascular tree secondary to rapid preoperative parenchymal shift and sudden increase in cerebral blood flow with focal disruption of autoregulation are the most probable explanations. Elderly patients with physiological aging of the small blood vessels associated with increased fragility may not tolerate a rapid normalization of the blood flow in areas of impaired cerebral vascular autoregulation.1112) In our patient, a brain CT scan after surgery showed multipunctate ICHs with SAH in both cerebral hemispheres. However, a preoperative DWI scan failed to show acute ischemic lesions due to compression of the brain by CSDH nor did a preoperative GRE scan reveal undetected areas of the cerebral contusion. Therefore, we suppose that the combination of rapid brain shift related to the prompt expansion of brain after sudden decompression and diffuse cortical hyperemia due to being accelerated by hyperperfusion were responsible for a SAH developing in our patient.
To avoid this devastating complication, we recommend discharging the chronic extracerebral fluid collection slowly under a closed system without a physiologic saline irrigation. Several authors proposed that twist drill holes with closed drainage is the safest and most effective surgical technique.45) This procedure provides slow and complete decompression through gradual re-expansion of the brain and also prevents rapid dynamic intracranial changes that may risk the postoperative hematomas.49) However, it is not easy to predict these postoperative hemorrhages after evacuation of the CSDH. When such complications are suspected, an immediate brain CT scan is necessary.
Go to :
 XML Download
XML Download