

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The polytrauma patients with severe head injury have a high mortality rate. Watson and colleagues19) reported that 30% of patients with severe splenic injuries had accompanying severe traumatic brain injury (TBI) of Glasgow Coma Scale (GCS) score ≤8. Nonoperative treatment of blunt splenic injuries is supported in hemodynamically stable patients, but splenic injury, which caused hypotension, requires splenectomy.918)
We report a rare case of concurrent operation of craniectomy and splenectomy as initial treatment in severe traumatic head injury.
Go to : 
Case Report
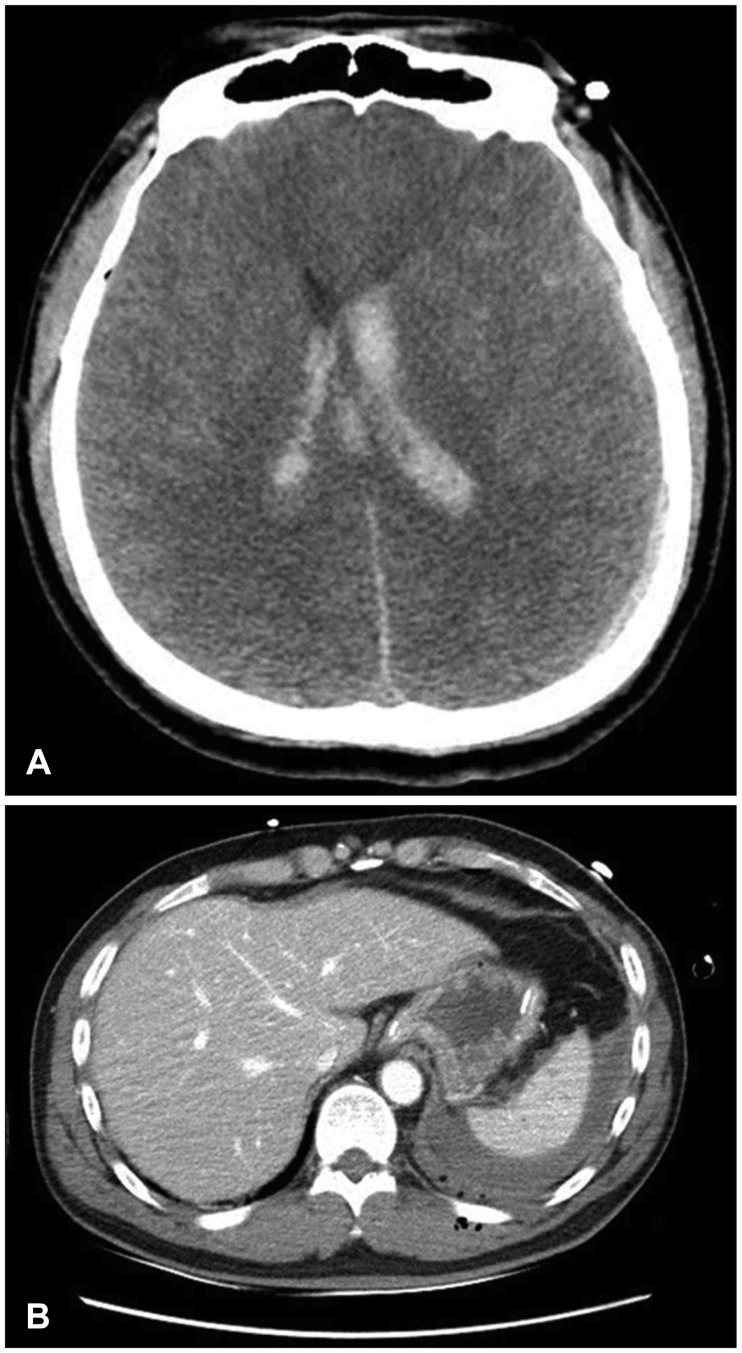
A 44-year-old man visited the trauma center with a motorcycle accident. The GCS score at the time of emergency department was 3 points, and pupils were fixed at 6 mm on both sides. He was unconscious, and hard to identify his medical history. Initial blood pressure (BP) was 135/85 mmHg, heart rate (HR) was 100 times/min, respiratory rate was 24 times/min, body temperature was 37.6℃ (99.68°F), and oxygen saturation was 95%. Also, it was identified that hemoglobin, hematocrit and platelet counts were 14.2 g/dL, 42.5% and 350×103/µL at laboratory test. Associated injuries included multiple fractures of whole body. Brain computed tomography (CT) revealed subarachnoid hemorrhage, intraventricular hemorrhage and severe cerebral edema and a small amount of hemoperitoneum was detected in abdominal CT (Figure 1).
During the preparation of the craniectomy in the operating room, BP was checked to 85/50 mmHg and HR was changed 131 times/min, and abdominal ultrasonography was performed emergently. As the result of that, a large amount of hemoperitoneum was confirmed. The blood tests at that time showed that hemoglobin and hematocrit dropped to 8 g/dL and 23.1%.
Hemoperitoneum was found to be the cause of hemodynamically unstable condition, and decompressive craniectomy was also urgently required to control cerebral edema and intracranial pressure (ICP). The bi-coronal craniectomy with duroplasty and splenectomy with vessel ligation were carried out simultaneously for about 4 hours. Because neurosurgeons and trauma surgeons had difficulty in secure their surgical space at the same time, the modified Mayo stand was installed. The surgery was well done under the close observation of the anesthesiologist (Figure 2). After fifty days of treatment, he was discharged with Glasgow Outcome Scale-extended (GOS-E) 4 points and is undergoing rehabilitation therapy.

Go to :
Discussion
Severe trauma is the main cause of death among younger people. Annual deaths worldwide due to trauma are expected to increase from five million to more than eight million by 2020.10)
TBI contributes to immediate and complicated physiologic changes, including cerebral hemodynamics instability and elevated ICP. These changes cause secondary insults and unfavorable outcomes in TBI patients.8) Also, cardiovascular abnormality in severe head trauma have been well known.4) Sympathetic nervous hyperactivity as measured by plasma and urinary epinephrine and norepinephrine levels has been verified in brain injury and in other medical conditions.720) After TBI, hypotension, hypoxia and hypercapnia have been shown to result in secondary brain injury that can lead to increased mortality and disability.2) It is important to find out the main cause that the vital signs became unstable, because the prognosis of patients with severe TBI and a low GCS score depends on how early the essential function is supported.16)
The spleen is the most common injured organ by blunt abdominal trauma, especially when it is already pathologically enlarged.13) In most of the 20th century, splenectomy was the treatment of choice for splenic damages.12) Recently, many investigators have reported that their good results with nonoperative treatment in children and adults and in hemodynamically stable patients.318) Alabbasi et al.1) reported analysis to evaluate two strategies (instant splenectomy and nonoperative management) for managing hemodynamically stable patients with blunt splenic injuries and severe brain injury.1) The overwhelming post-splenectomy sepsis syndrome is one of the main reasons for the increased emphasis on splenic conservation in current literature. It is a frequent and acute complication with an incidence of up to 1% after splenectomy, and an associated mortality of 50% to 70%.17) The decision on the surgical treatment strategy depended on the severity-level of the splenic damage, on associated injuries as well as the cardiovascular situation of the patient.6)
Uncontrolled post-traumatic bleeding is the cause of potentially preventable death among injured patients.14) As a result of only head trauma as well as polytrauma, cerebral blood flow (CBF) irregularities vary abnormally from low to high.11) Low CBF leads to decreased brain metabolism and ischemia, whereas increased CBF deteriorates brain swelling and high ICP.15)
Hildebrand et al.6) suggested the surgical treatment in a hemodynamically instable patient with grade 2 or greater splenic injury through the therapy algorithm. Surgical treatment of brain injury was also required to control cerebral edema and ICP and to prevent secondary brain damages. Our case report demonstrates the first experience of simultaneous surgery for reasons of hemodynamical and neurological deterioration.
In 2009, Goldschlager et al.5) reported a case of simultaneous craniotomy and caesarean section on extreme situation of trauma.
Go to :
 XML Download
XML Download