

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Osteoporotic vertebral compression fractures (VCF) in thoracic and lumbar vertebrae are a common injury in elderly patients. The vast majority of compression fractures in elderly patients are caused by low-energy trauma, and are stable because only the anterior column is involved. This injury can be effectively treated with conservative treatment, including medication, bed rest, and external orthosis.8121424273132)
Although there have been controversies, percutaneous vertebroplasty (PVP) has been a good treatment option in patients who were unresponsive to those conservative treatments.137810121926283031) However, there are no firm guidelines on how long or how we should undertake conservative treatment during the acute period of compression fracture.719) We hypothesized that if a strong analgesic medication was used, including opioids, and a corset brace instead of a bulky plastic brace to make higher compliance, convenience, and less cost, we could increase the success rate of conservative treatment, which would result in a reduction of subsequent PVP. In addition, we presumed that early ambulation to a toilet, thereby removing the absolute bed rest period, would be helpful for avoiding patient morbidity. Thus, this study was performed retrospectively to determine the success rate of our conservative treatment method for VCF and to find its prognostic factor.
Go to : 
Materials and Methods
Patient population and inclusion criteria
We retrospectively performed conservative treatment with the same protocol in 82 eligible patients with an osteoporotic compression fracture in a single center from March 2012 to August 2015. However, in this study, we only included patients with a single level VCF developed within 3 days and without a history of previous vertebra fracture treatment or the presence of medical comorbidity. The other inclusion criteria of patients were being aged more than 55 years old, the presence of localized back pain without any motor or sensory deficit correlated with magnetic resonance image (MRI), all agreed VCF with bone edema by a radiologist and a neurosurgeon with MRI, acute onset lower energy trauma, such as slip down or spontaneous back pain, visiting through the outpatient clinic or the emergency medical center, with a possible follow-up of more than 1 year. Patients whose T-score of bone mineral density (BMD) on spine was less than −1.0 were included in this study.
High-energy trauma-suspected injuries, including traffic accidents, falling down from a high place, or an industrial accident, were excluded. Other exclusion criteria were medical comorbidity, the presence of coagulopathy, a systemic or local spine infection, a suspected pathologic fracture, the retropulsion of bony fragments, combined with another fracture, combined radiculopathy or myelopathy, previous VCF history with or without PVP, multiple compression fractures, impossible follow-up at 1 year, the presence of any psychiatric disorder, and difficulty in communicating. On the basis of those criteria, and after removing 7 patients whose follow-up was lost, 75 patients (22 male and 53 female) whose mean age was 70.5 years old were included in the final analysis.
Treatment protocol
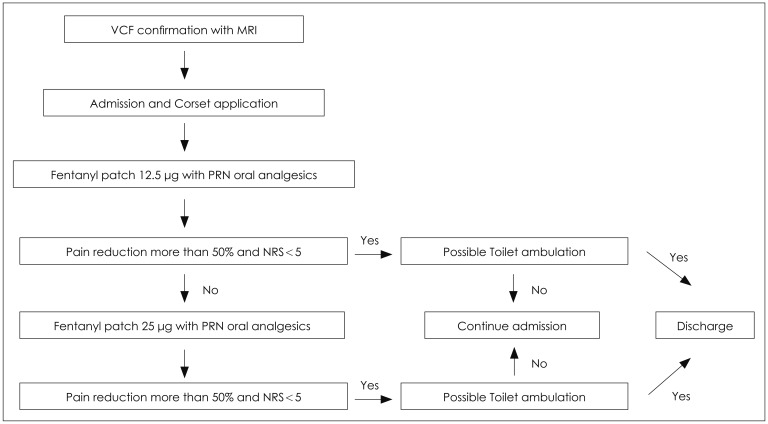
An MRI was performed and admission and osteoporosis medication were recommended in all patients. We recommended at least 3 month corset application in all patients except four with thoracic lumbar orthosis (TLO) due to an above T8-level fracture. After admission, a transdermal fentanyl patch with a low dose (12.5 µg) application was attempted in all patients. A tramadol 37.5 mg/acetaminophen 325 mg combination tablet or an acetaminophen 250 mg, ibuprofen 200 mg, and codeine phosphate 10 mg combination tablet were prescribed as a pro re nata (PRN) oral medication. Patients were advised that side effects, such as nausea or dizziness, might develop because of the fentanyl patch. When such a side effect developed, even in the use of a low-dose fentanyl patch in 13 patients, we removed it from their medication and used only oral analgesics instead. After the low-dose fentanyl patch application, the patients were asked if there was a change in their pain numeric rating scale (NRS). If it decreased below 5 or was 50% below the initial NRS, we continued to use the low-dose fentanyl patch for 1 month. However, if the patient complained of sustained pain more than NRS 5% or 50% of the initial pain NRS, we increased the dose of the fentanyl patch by 25 µg. After identifying a tolerable toilet ambulation of the patient without any assistance, hospital discharge was recommended. We followed patients at the outpatient clinic over 1, 3, 6, and 12 months. Although we tried to cut off the fentanyl patch after 1 month and prescribe only PRN oral analgesics during follow-up, five patients found it necessary to retain the patch for 2 months (Figure 1).
Outcome analysis
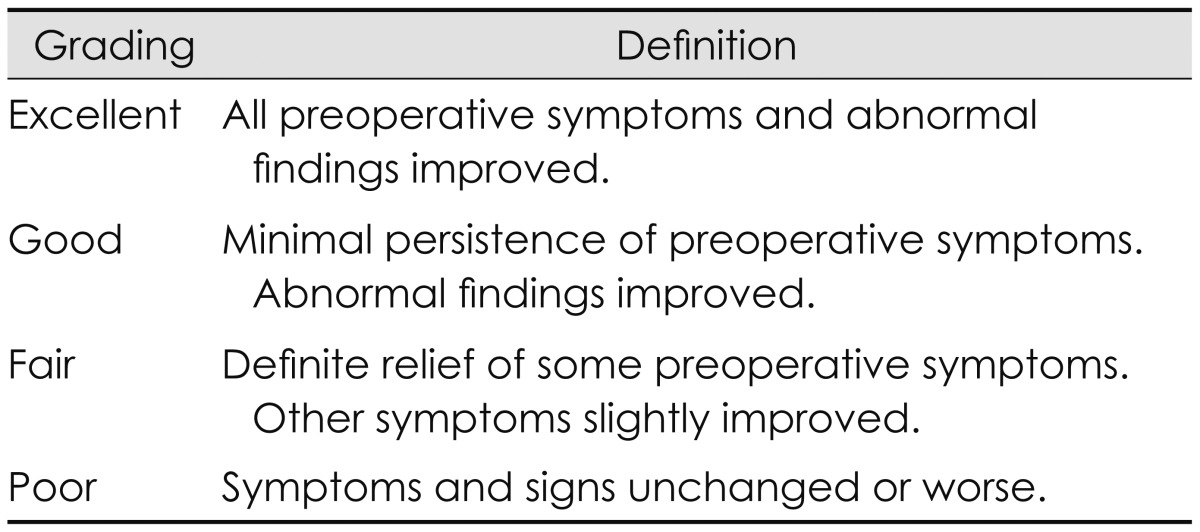
We collected the pain NRS at the initial state, 3, 6, and 12 months and short form-36 (SF-36) physical component summary (PCS) at initial state and 12 months. In addition, we surveyed Odom's criteria at 12 months.20) Excellent and good in Odom's criteria were regarded as satisfied patients, and fair and poor were regarded as unsatisfied. During follow-up, six patients had PVP performed at a different hospital. We classified two patient groups: favorable with satisfied patients, and unfavorable with unsatisfied patients and six patients who had had PVP performed (Table 1).
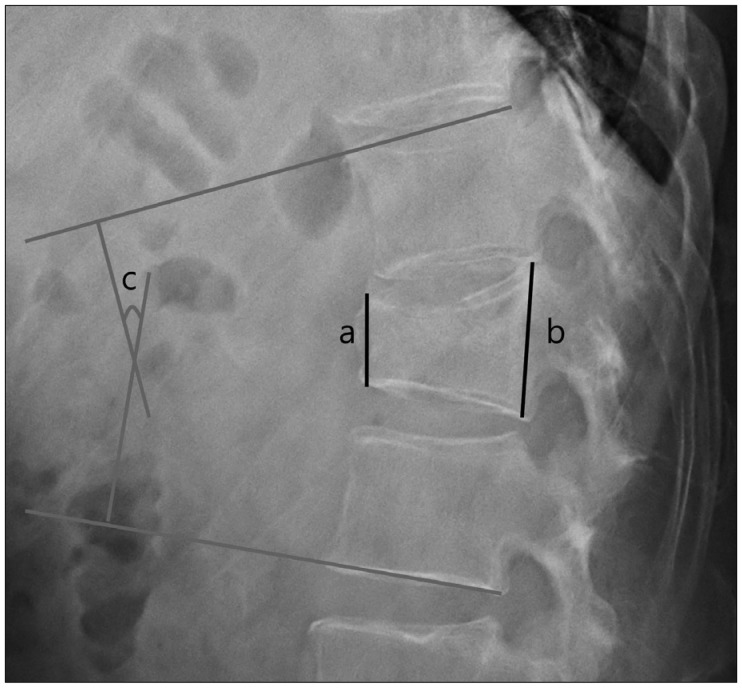
Radiological X-ray follow-up was done at the initial state, and at 1, 3, 6, and 12 months. The compression rate and Cobb angle was measured during follow-up (Figure 2).
We compared basic characteristics, clinical outcome such as NRS and SF-36, hospital stay, the duration to return to usual normal activity, the dose of used patch, and radiological outcomes such as compression rate and Cobb angle.
Student's t-test, the Fisher's exact test, the Mann-Whitney U test, and the linear mixed model for statistical analysis were used.
Go to :
Results
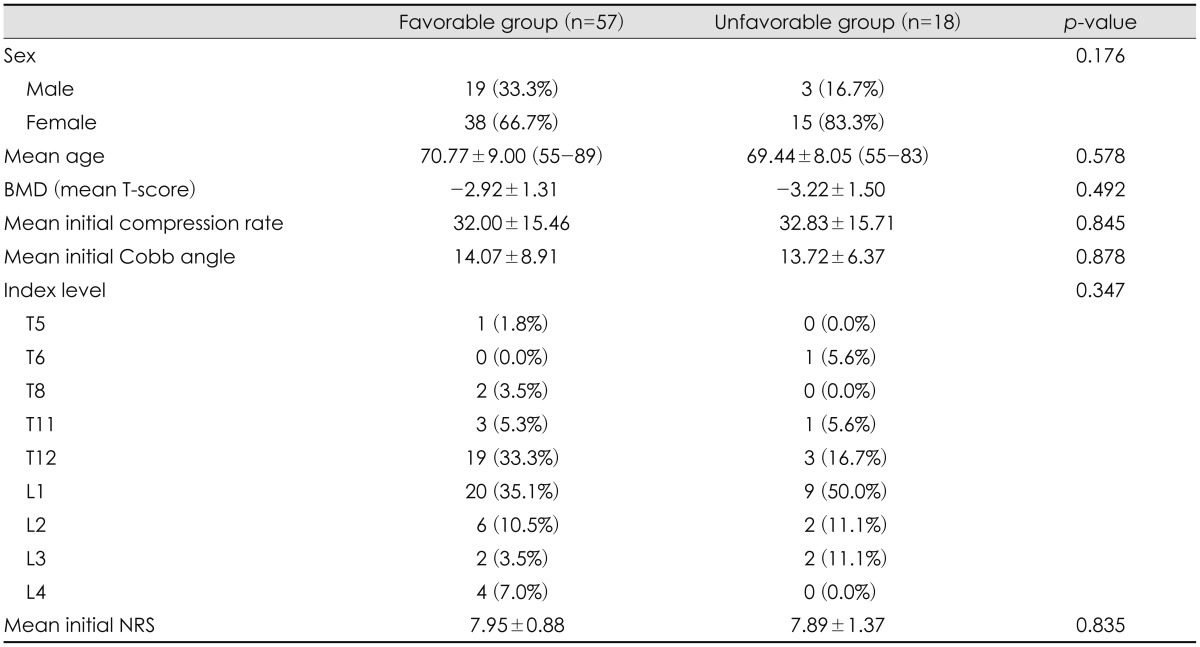
Among 75 patients, the clinical outcome of 57 (76%) was favorable, but that of 18 (24%) was unfavorable, which included 12 unsatisfied patients and 6 patients undertaken PVP at a different hospital. The basic characteristics including sex, age, BMD, initial Cobb angle and compression rate, index level, and initial NRS were not statistically different between the favorable and unfavorable groups (Table 2).
In the clinical outcome, NRS at 6 and 12 months and Odom's criteria at 12 months were significantly different between the favorable and unfavorable groups (Table 3).
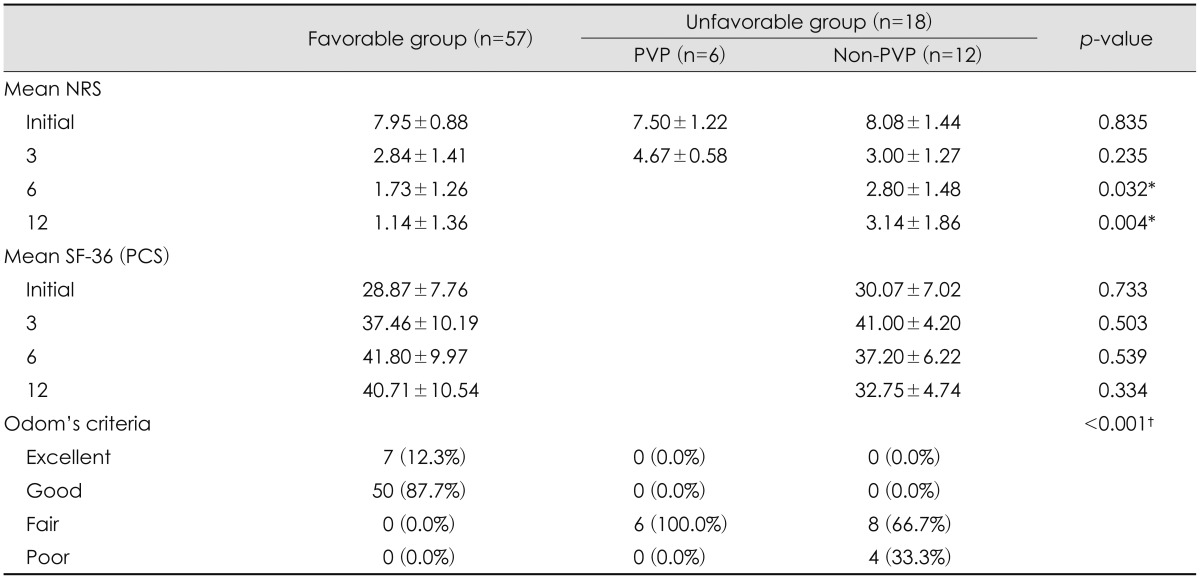
TABLE 3
Comparison of clinical outcomes between favorable and unfavorable groups
The data is presented as n (%) or mean±standard deviation. *Means statistically significant (Student's t-test was used to examine the degree of difference between the two groups), †means statistically significant (Mann-Whitney U test was used to examine the degree of difference between the two groups). PVP: percutaneous vertebroplasty, NRS: numeric rating scale, SF-36: short form-36, PCS: physical component summary
![]()
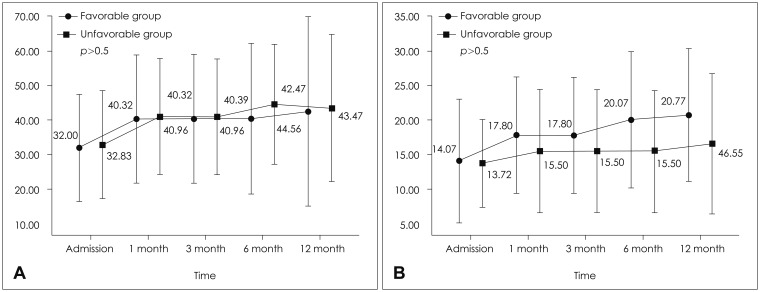
In the radiological outcome, the compression rate increased until 1 month, but showed a steady state from then onwards. There was no statistically significant difference between the two groups in all assessment time points (Figure 3A). The Cobb angle increased until 1 month, but showed a steady state until 3 months and increased again until 6 months in the favorable group. That of the unfavorable group increased until 1 month and showed a steady state until 12 months. There was also no statistically significant difference between the two groups in all assessment time points (Figure 3B).
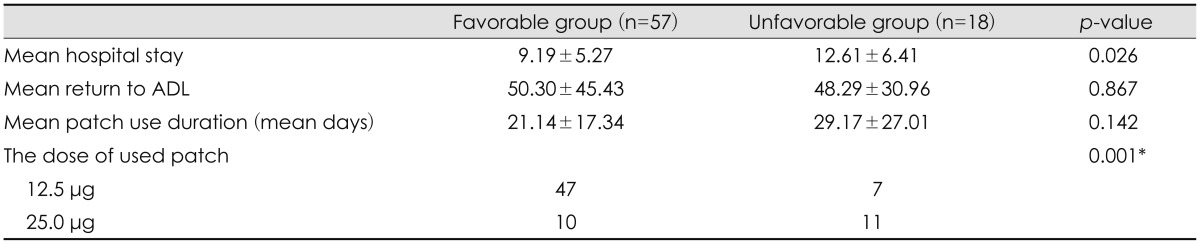
Regarding hospital stay, return to activity of daily living (ADL), patch use duration, and the dose of the patch used, only the dose of the patch used showed a statistically significant difference between the favorable and unfavorable groups (p=0.001) (Table 4).
There was no adverse event during our treatment protocol, such as pulmonary dysfunction or deep vein thrombosis.
Go to :
Discussion
Traditional treatment for VCF includes oral analgesics, an external brace, and bed rest.7812141924273132) However, any guidelines of conservative treatment have not been suggested.61216) Although one study suggested absolute bed rest, it could be related to pulmonary dysfunction, deep vein thrombosis, muscle atrophy, pressure sores, sleep disorders, and depression.48) These reasons led us to avoid absolute bed rest and encourage the patients to ambulate early. Thus, we could achieve shorter hospital stay (Table 4) compared to a previous study despite similar clinical result.4) In comparing our compression rate in Figure 3A to the previous study, our progression of the mean compression rate was nearly 10% and a little more progressive (10% vs. 7%).4) Although we agree that this might be caused by relatively early ambulation, we believe that its benefit to avoid complications related with longer bed rest weigh on a little more than subtle progression of compression rate.
Although analgesia (e.g. paracetamol, salicylates, and non-steroidal anti-inflammatory drugs [NSAIDs]) has been recommended as a first-line medication, the risk of gastrointestinal bleeding and renal insufficiency should be taken into account when prescribing NSAIDs.1618) Opioids, such as oxycodone combined with paracetamol, can be administered for patients failing to obtain adequate relief from first-line medications. However, narcotics have significant side effects, including reduced gastrointestinal motility, urinary retention, reduced respiratory drive, and cognitive deficits with loss of balance, an increase in falls, and depression.51621) Because of the development of those possible side effects, we had to recommend that all patients be admitted to the hospital and use individual fentanyl patches under careful monitoring. We could not use fentanyl patches on 13 patients because of nausea and dizziness; however, no patients had a reduction in respiratory drive. Previously, we have shown the efficacy and safety of fentanyl patch use in chronic pain.21) Fentanyl patch offers an interesting alternative to oral morphine, and its effectiveness and tolerability were demonstrated by several trials.9) In general, fentanyl patch has the same adverse effects as other opioids, mainly sedation, nausea, vomiting, and constipation. In comparison with oral morphine, it causes fewer gastrointestinal adverse events. The risk of hypoventilation is comparatively low in patients with cancer. In addition to safety and our experience, the most important reason to choose fentanyl patches instead of other oral opioids was the convenience of changing them every 3 days. Because of a concern for safety, we did not want to increase the dose above 25 µg and the compliance of patients was good. Although the consideration of the abuse and addiction of fentanyl led us to stop it possibly up until 1 month's use, it was necessary to continue it for a relatively long duration (until 3 months) in five patients.
Wearing a brace is important in the conservative care of VCF. The primary goal of bracing is to reduce pain by stabilizing the spine and limiting progression of the kyphosis. Braces can help to reduce movement at the level of the fractured vertebra and thus allow bone healing. Moreover, bracing allows a reduction in the period of bed rest, facilitating earlier mobilization.111625) Although traditionally, the braces were three-point contact rigid plastic braces (e.g. the TLO or the lumbar sacral orthosis brace) were superiorly advocated,21316172223) some authors recommended a corset instead.1629) We only intended to improve the compliance of patients, due to lower compliance of uncomfortable bulky plastic brace.1617)
The indications for PVP, including kyphoplasty, remain controversial, but they can be an option in patients whose conservative treatment failed. The comparisons between these two procedures have remained equivocal, until now.3610121531) However, our results showed an unfavorable outcome in 18 patients (24%) after conservative treatment. Thus, we agree that some proportion of patients might be more favorable if we could perform PVP after the acute period. Considering the results of this study, as higher dose of fentanyl patch was associated with unfavorable outcome after the conservative treatment, the dose of fentanyl patch seems to be helpful in discriminating between favorable and unfavorable patients during the acute conservative treatment period. And this can help to make proper decision for whom PVP should be performed. The reason we suspected that the different dose of patch could discriminate an unfavorable outcome was that it depends on different pain sensitivity according to different people. A patient who is more sensitive to the pain might tend to get PVP at a different hospital or to complain of a longer period sustained pain.
Our study has several limitations, including a small patient population and no comparison group. Further well-designed comparative studies are necessary to show the efficacy of the fentanyl patch for the conservative treatment of VCF.
Go to :
Conclusion
We showed the outcomes of conservative treatment in the 75 VCF patients with use of the fentanyl patch as the first-line medication. Among the 75 patients, the clinical outcome of 57 (76%) was favorable, but in 18 (24%) was unfavorable. The only statistically significant prognostic factor for an unfavorable outcome was the use of a higher dose fentanyl patch. Our data infer that the unresponsiveness to a low-dose fentanyl patch could be helpful to select patients for the PVP or kyphoplasty after conservative treatment.
Go to :
 XML Download
XML Download