

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Various surgical techniques can be used for the treatment of degenerative cervical disease caused radicular pain secondary to the soft disc heniation or foraminal stenosis.914151824) Although anterior cervical discectomy and fusion (ACDF) is widely accepted the gold standard for the management of cervical radiculopathy at the present time, posterior cervical foraminotomy has been recommended as an effective surgical treatment option in appropriately selected patients.3924) In addition, this technique has several advantages over anterior cervical discectomy such as easy root decompression, avoidance of major neck structures, preservation of motion segment and avoidance of potential morbidities associated with arthrodesis.1723)
However, the more wide extent of foraminal pathology, the more extensive laminoforaminotomy may be required. Furthermore, too excessive facetectomy becomes associated with a higher risk of instability.517) The present study was performed to compare retrospectively the clinical parameters and surgical outcomes of posterior cervical laminoforaminotomy between soft disc herniation and foraminal stenosis patients in the treatment of cervical radiculopathy.
Go to : 
Materials and Methods
Patients and evaluation
A total of 47 patients who managed by laminoforaminotomy at a single level unilaterally for cervical radiculopathy were retrospectively reviewed between 2004 and 2012 in a single institute. Mean follow up period was 16.3±8.2 months. We classified 47 patients into two groups based on the disease: Group A for soft ruptured disc (n=27) and Group B for foraminal stenosis patients (n=20). Then, we compared the demographic factors, amount of medial facetectomy, postoperative instability with neck pain and clinical outcomes between the two groups.
Inclusion criterias were posterolaterally located soft ruptured disc, foraminal stenosis secondary to bony spurs, facet arthropathy with foraminal compression and continued radiculopathy after ACDF.
The patients with significant central canal stenosis, alignment abnormalities, or myelopathy were excluded.
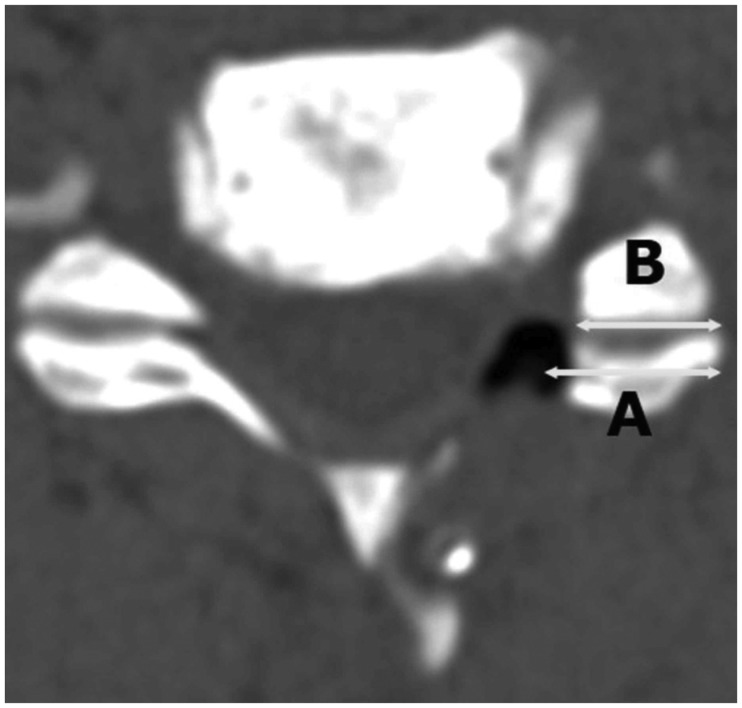
All patients had preoperative evaluation with static (anterior-posterior and lateral) and dynamic (flexion/extension) plain cervical spine radiography, computed tomography (CT) and magnetic resonance imaging. All patients were assessed the instability using dynamic plain cervical radiography at 1years postoperatively and reviewed the extent of medial facetectomy by immediate postoperative CT. In postoperative CT, we measured A: length of contralateral facet and B: length of remnant facet and then, the percentage of facetectomy was calculated as follow, Facetectomy (%)=(A−B)×100/A (Figure 1).
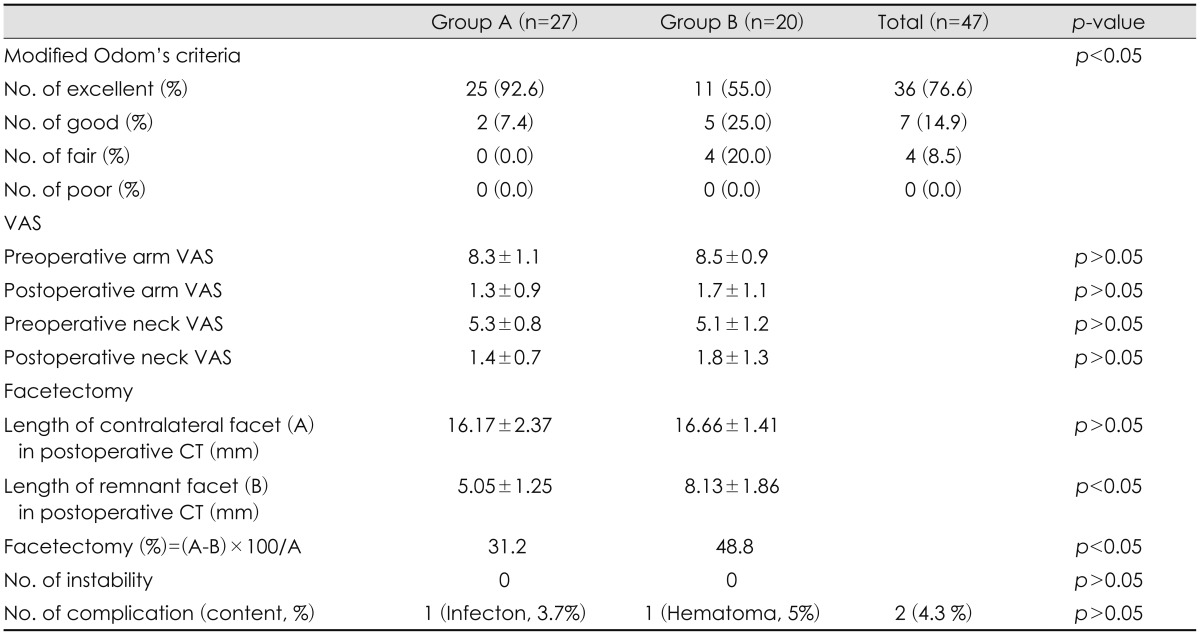
The preoperative and postoperative visual analogue scale (VAS) scores of neck and arm pain and modified Odom's criteria (Table 1) for surgical outcomes were evaluated for clinical assessment.

Surgical technique
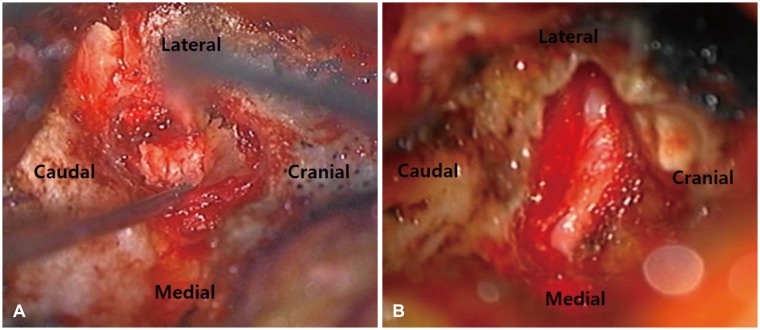
All patients were operated on in a prone position. The patient is positioned in slight flexion using the horseshoe headrest and the neck is maintained parallel to the floor to minimize epidural venous bleeding and risk of air embolism. A vertical 3 to 4 cm midline incision was made after obtaining a lateral radiograph to confirm the correct operative level. Under a surgical microscope, a partial hemilaminectomy and partial facetectomy was performed using various punches and high-speed drills following the exposure of lateral lamina and medial facet joints. The extent of the facet resection was based on the extent of the foraminal pathology until medial half of the facet joint. In cases of soft disc herniation, the proximal root was adequately visualized in order to remove the compressing disc material. However, in cases of foraminal stenosis, the adequate decompression of the proximal root needs to be further assessed carefully using a 2 or 3 mm diameter diamond burr, microcurette and punch. Patients wore a soft collar for 4 weeks after the operation and were given adequate medication (Figure 2).
Statistical analysis
The SPSS 12.0 statistical software package (SPSS, Inc., Chicago, IL, USA) was used for statistical analysis. Data were analyzed using the χ2 and Student's t-tests, as appropriate. A p-value of <0.05 was considered to be statistically significant.
Go to :
Results
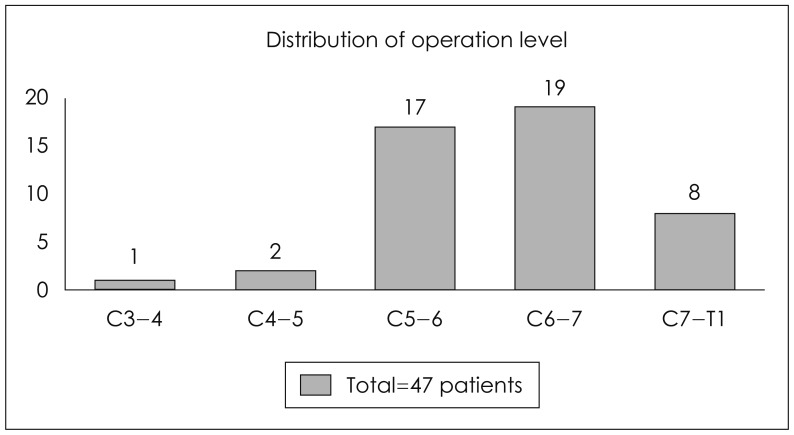
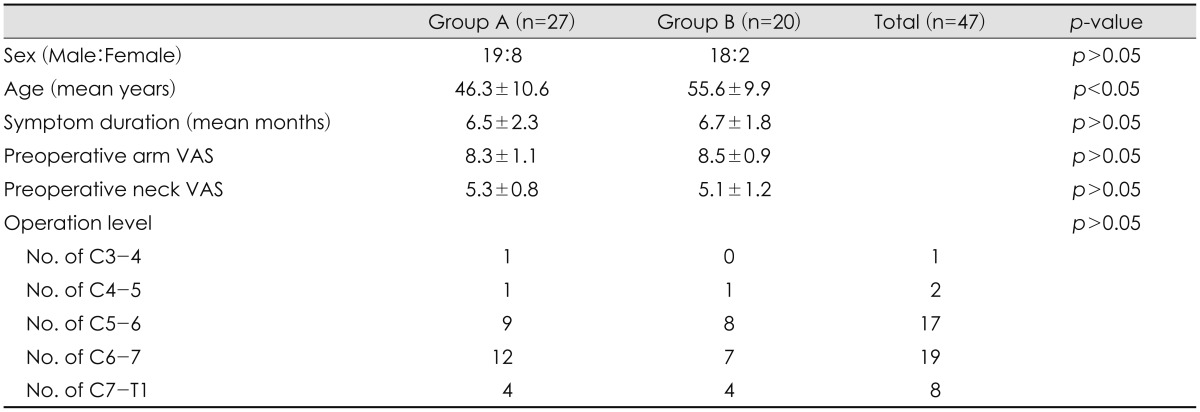
As for the our results, there were statistically no difference between two groups in sex, preoperative symptom duration and preoperative VAS score. But there was difference in mean ages. The most frequent operation level is C6–7 and the next is C5–6 (Table 2 and Figure 3).
According to the modified Odom's criteria, laminoforaminotomy for the ruptured disc showed surgical success rate (good or excellent) in 100% (92.6% excellent and 7.4% good results) of patients and for the foraminal stenosis in 80% (55.0% excellent and 25.0% good results), which was statistically significant (p<0.05). However, when including both groups. Overall success rate showed in 91.5% of patients (Figure 4).
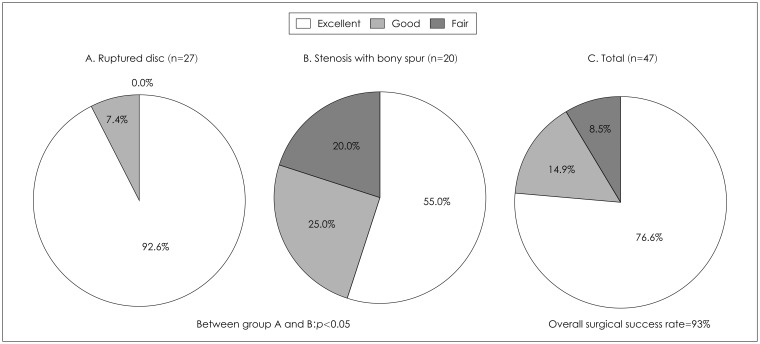 | FIGURE 4(A) According to the modified Odom's criteria, laminoforaminotomy for the ruptured disc showed 92.6% excellent results and (B) for the foraminal stenosis was 55.0% excellent and 25.0% good results, which was statistically significant (p<0.05). (C) However, when including both groups. overall success rate showed 91.5%.
|
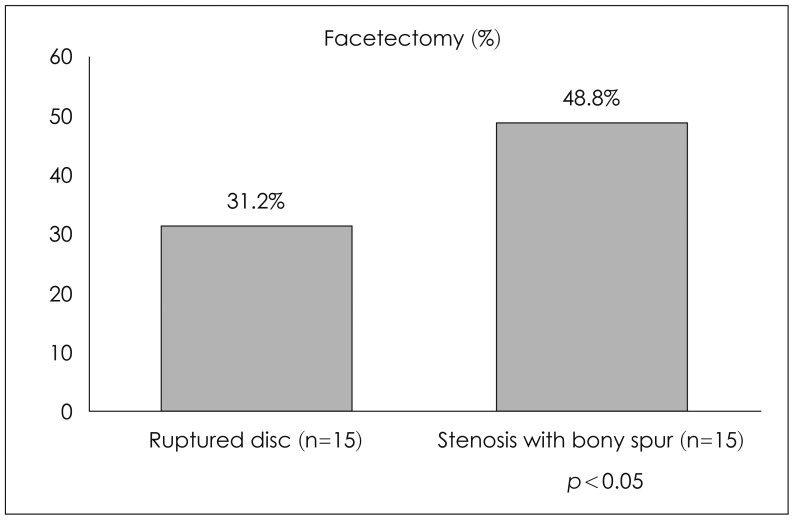
Although posterior laminoforaminotomy for the ruptured disc showed the better outcomes than foraminal stenosis, The extent of medial facetectomy for ruptured disc (5.05±1.25 mm, 31.2%) was smaller than for stenosis (8.13±1.86 mm, 48.8%) and it was statistically significant (p<0.05) (Figure 5).
Postoperative mean arm and neck VAS were markedly decreased compared with preoperative arm and neck VAS in both groups. But, 13 patients complained of postoperative neck pain. Group A was 6 patients (22.2%) and Group B was 7 patients (35.0%). There was no statistically significance. And this symptoms were resolved about 2 months after operation spontaneously.
There was no instability on dynamic X-ray until the last follow up period and we had two cases complications (4.3%). One of them was spondylodiscitis and the other one was postoperative hematoma. Spondylodiscitis was managed by antibiotics and postoperative hematoma was absorbed spontaneously. These results were summarized in Table 3.
Go to :
Discussion
The posterior approach to cervical pathology was originally introduced by Mixter and Barr. Subsequently, the keyhole foraminotomy was popularized by Scovill, Epstein, and Fager. Ducker renamed it to the term laminoforaminotomy later.6824) However, the technique was increasingly replaced by the anterior cervical approach with or without fusion due to the ease of exposure and wider exposure of the disc space.19) Although anterior cervical surgery is generally indicated for the management of midline or paramedian discs or spurs.1120) The treatment of lateral or foraminal pathology by the anterior or posterior approaches remains controversial.10)
The major advantages of laminoforaminotomy versus anterior approaches are easy root decompression, avoidance of major neck structures, preservation of disc and motion segment and avoidance of potential morbidities associated with arthrodesis.1723) However, following laminoforaminotomies, some patients have a severe postoperative neck pain and muscle spasm, possible instability after facetectomy. Also, perineural and epidural bleeding can obscure surgical field.517)
In many previous report,19121624) posterior laminoforaminotomy has been showed favor surgical results in 82% to 97% of patients who have cervical radiculopathy caused by foraminal stenosis or posterolateral herniated discs. Henderson et al.9) published a comprehensive review of 846 surgical cases performed in 736 consecutively treated patients with cervical radiculopathy using the laminoforaminotomy technique. Good or excellent outcomes were obtained in 91.5% of patients and there was no statistically significant difference between the outcomes for patients with hard or soft disc herniation or cervical spondylosis. However, Krupp et al.13) described that in according to Odom's classification, the average values obtained in soft disc cases were significantly better than those achieved in the group treated for a hard disc and Woertgen et al.22) observed bad outcomes were often observed in patients with bony foraminal stenosis. In our study, although overall good or excellent outcomes showed in 91.5% of patients, posterior laminoforaminotomy for the ruptured disc showed the better outcomes (100%) than foraminal stenosis (80%).
The percent of facet resection is based on the extent of foraminal pathology.7) Some previous studies241723) suggested that the extent of facet resection required during laminoforaminotomy is typically 25%, and rarely exceeds 50%. In Baba et al.2), 16 nerve roots were adequately exposed with 25% of the facet removed, while 8 patients required a 25% to 50% medial facetectomy. In Zdeblick et al.'s cadaveric study23), laminectomy alone did not allow visualization of the nerve root. The 25% facetectomy allowed visualization of mean 2.7 mm nerve root; 50% facetectomy, 5.9 mm; 75% facetectomy, 10.0 mm; 100% facetectomy, 14 mm. Similarly, Raynor et al.17) reported that 3 to 5 mm of root could be exposed with 50% facetectomy, and 8 to 10 mm with 70% facetectomy. However, 50% or more facet resection becomes associated with a higher risk of instability.1723) In our study, 31.2% medial facetectomy was enough for removing the posterolaterally located soft disc. On the other hand, 48.8% facetectomy in patients with foraminal stenosis showed lower clinical outcomes than soft disc.
Tanaka et al.21) reported that the shape of the intervertebral foramina approximated a funnel, the entrance zone being the most narrow part in cadaveric study. Therefore, compression of the nerve roots occurred at the entrance zone of the intervertebral foramina. This observation may suggest that in many cases of foraminal stenosis, medial facetectomy until the 50% was possible to decompress the nerve root sufficiently. However, we suggest that the location and extent of osteophyte, disc height, individual variation in the nerve root and three-dimensional foraminal anatomy might affect the surgical results of laminoforaminotomy in foraminal stenosis patients.
According to our study, the posterior cervical laminoforaminotomy for posterolateral soft disc is a comparable surgical option with ACDF. However, in the case of cervical foraminal stenosis, more precise comparison with anterior approaches is necessary from the point of clinical outcomes and radiological changes.
Go to :
Conclusion
Posterior laminoforaminotomy is an effective procedure for radiculopathy with laterally located soft disc or spondylotic foraminal stenosis. The extent of facetectomy for ruptured disc was smaller than it for stenosis. Posterior laminoforaminotomy for the ruptured disc showed the better outcomes than foraminal stenosis, but overall success rate of posterior foraminotomy was 91.5% and complication rate was 4.3%.
Go to :
 XML Download
XML Download