

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Traumatic brain injury (TBI) is defined as an acute injury to the head caused by blunt or penetrating trauma or from acceleration/deceleration forces excluding degenerative, congenital problems.1849) Glasgow Coma Scale (GCS) score is used in grading TBI; mild TBI (GCS 13-15) is in cases of alert and drowsy mentality and most recovers well without neurologic deficit, moderate TBI (GCS 9-13) lethargic or stuporous patients are categorized and in severe injury, severe TBI (GCS 3-8) the patients are in comatous, unresponsiveness to external stimulations.17) TBI is a major health problem worldwide, with an estimated 10 million cases leading to hospitalization or death each year.36) It is the most common cause of death and disability in children and young adults.2) In the United States, TBI affects 1.5 million people, resulting in 235,000 hospitalizations, 50,000 deaths, and permanent disability in 99,000 people per year.242)
Normal intracranial pressure (ICP) in adults is below 15 mmHg. If it is maintained above 20 mmHg in patients with TBI, it is determined to be pathological and appropriate adjustment is necessary. According to Monro-Kellie doctrine, “the sum of the intracranial volumes of blood, brain, cerebrospinal fluid (CSF) and other components is constant and that an increase in any one of these must be offset by an equal decrease in another.”314054) The volume of these compartments is tightly regulated, and cerebral blood flow (CBF) is kept constant by autoregulation. When the physiologic equilibrium had broken by adding additional volume to the system, compensatory mechanisms operate to keep ICP constant.47) In patients with severe TBI, autoregulation does not work due to pathologic increase in ICP that may compromise cerebral perfusion pressure (CPP) and lead to neurologic deterioration and fatal brain herniations. Medical treatments are used in control ICP including head elevation, intubation for normocarbic ventilation, sedation, hyperosmolar therapy by mannitol or hypertonic saline, induced hypocapnia, hypothermia and metabolic suppression by barbiturates. Surgical treatments including ventricular CSF drainage and decompressive craniectomy (DC) also be effective.47)
DC had been used to control ICP associated with abnormal conditions, including intracranial neoplasm, ischemic disease, and diffuse edema from TBI. The benefit of DC in the treatment of malignant infarction had been proved by previous studies.202851) Although DC in TBI reduce ICP by evacuate hematoma and provide wider space for brain, its improvement for clinical outcome is not clear. In a randomized controlled trial (RCT) reported Cooper et al.9) suggested DC did not significantly improve clinical outcomes, despite of its effective reduction of ICP. In this article, we summarized the overall reviews of DC including historical base, surgical methodology, rationale, complications and recent clinical studies.
Go to : 
Historical Backgrounds
In B.C. 4000 Ancient Incas trepanned the skull for therapeutic or superstitious reasons.8) This is the first cranial surgery recorded in human history. Evidence of surgical decompression performed to treat TBI also found in Ancient Egypt and Greece.1438) Since then six centuries, Gallen introduced anatomy and better plans to evolve the procedure for describing indications for traumatic brain lesions including hematoma and fracture.35) In the modern era, Annandale in 1894, first described DC as a procedure and through the 19th century neurosurgeons performed craniectomy for palliative reasons.1144) Kocher33) in 1901, proposed DC for patients with raised ICP due to TBI and Cushing13) described DC to relieve ICP. This was employed in the management of inoperable brain tumors, but Cushing went further utilizing DC in the treatment of other brain disorders including post traumatic brain edema and vascular malformations.29)
Until the late 1960s and 1970s, DC was not welcomed due to its poor clinical outcome after surgery and the experimental evidence showed DC worsen brain edema.10) At that time, there was no clearance in benefit of surgical outcome and several groups began to research about specific decompressive techniques for the treatment of severe TBI. Jamieson and Yelland24) in 1968, reported results for successful surgical treatment of traumatic epidural hematomas (EDHs), with a mortality rate of just 16% in a series of 167 patients. In 1972, they reported surgical outcome of traumatic subdural hematoma (SDH).25) However, the outcome was poor with an associated 43% mortality rate in a case of 317 patients underwent a DC. Similarly, surgically managed traumatic intracranial hematomas in 63 cases were associated with a 24% mortality rate.26) In 1971, Kjellberg and Prieto32) reported 73 cases (50 cases with TBI), using a bifrontal DC with duroplasty for severe brain edema. The survival rate was 18% among them (22% in cases of TBI), as well as an additional 16 patients who showed neurological improvement after surgery but died due to other complications. In 1971, Ransohoff and Benjamin44) reported the result of treatment of SDH by a wide decompressive hemicraniectomy (DHC) with durotomy, which resulted in 40% of survival rate, and 28% of patients returning to preoperative condition. These outcomes were much improved over an 85% mortality rate among TBI patients treated with small craniectomies or burr holes. In 1975, Venes and Collins52) reported retrospective analysis of 13 patients who had bifrontal DC after TBI with severe brain edema. They showed a significant decrease in mortality (31%), but the morbidity was too much severe among the survivors, and only one patient (a child with moderate to severe TBI) returned to normal neurological function postoperatively.
After the 1980's there were many questions about the usefulness of DC, but the research continued. In 1980, Gerl and Tavan16) reported that extensive bilateral DC with durotomy offers the possibility of rapid reduction of ICP. According to the results, 70% of patients were died and 20% of the cases were recovered. In 1990, Gaab et al.15) performed a prospective study with 37 patients younger than 40 years old, they performed 19 bifrontal craniectomies and 18 hemicranietomies. They reported 5 cases of mortality, all others achieved full recovery or remained moderately disabled. The treatment outcome was most affected by the initial posttraumatic GCS ≥7.
Recently, DC has been increasing, therefore many papers published about the therapeutic effect. Unfortunately, most of them are mainly retrospective reviews with limited number of cases. In 2009, Hofmeijer et al.20) reported RCT of surgical decompression for space-occupying cerebral infraction and showed DC reduced case fatality and poor outcome in patients with malignant infarctions who are treated within 48 hours of stroke onset. On the other hand RCT designed for DC in TBI performed by Cooper et al.9) showed no favorable outcomes. All of these studies showed a rising concern for the utility of DC for TBI and provide evidence for a possible benefit regarding mortality rate after surgical decompression in severe TBI but questioned whether the morbidity and disability attained are justifiable. Importantly, the complex nature of TBI was recognized more than just the surgical aspects of management.
Go to :
Methodology of DC
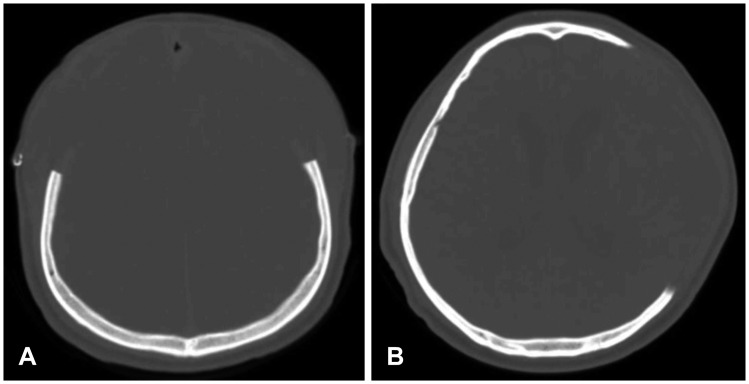
The main role of DC in TBI is reduction of ICP and prevention of herniation, aggravated by hematoma and brain swelling. DC must be extensive in all times, because the benefits of DC directly affected by surgical technique and degree of decompression achieved. Two main techniques widely used for DC in TBI are unilateral frontotemporoparietal craniectomy and bifrontal craniectomy (Figure 1). Unilateral frontotemporoparietal craniectomy is especially useful for unilateral localized lesion, including traumatic hematoma, brain swelling due to middle cerebral artery (MCA) infarction. The patient is placed supine position with head turned to contralateral side. The ideal sagittal angle of head is 0° to 15° horizontal to the floor.43) A large reverse question mark shape incision is made from the midline anterior to the coronal suture, posterior several centimeters behind the ear, and to the root of the zygoma. The midline should be clearly marked and the incision should be performed approximately 2 cm lateral to the midline for preventing damage to superior sagittal sinus (SSS). When we make the incision, superficial temporal artery (STA) located approximately 1 cm anterior to the tragus, should be careful. The bone flap should be more than 15 cm in anteroposterior diameter and should extend down toward the floor of the temporal fossa to provide adequate decompression.1) With small and inadequate size of decompression may cause further brain damage by compression of the brain cortex and cortical veins that enhancing brain herniation. This situation elevated the risk of contusions at the bone edge and may also have greater axonal strain.3753)
The location and number of burr holes depends on the preference of the surgeon, but typically four holes method are widely used; 1) Temporal squama, 2) Parietal area just posterior to the parietal bone and close to the skin incision, 3) Frontal area 2 cm in front of the coronal suture and close to the skin incision, 4) Key hole area behind the zygomatic arch of the frontal bone (Figure 2).43)
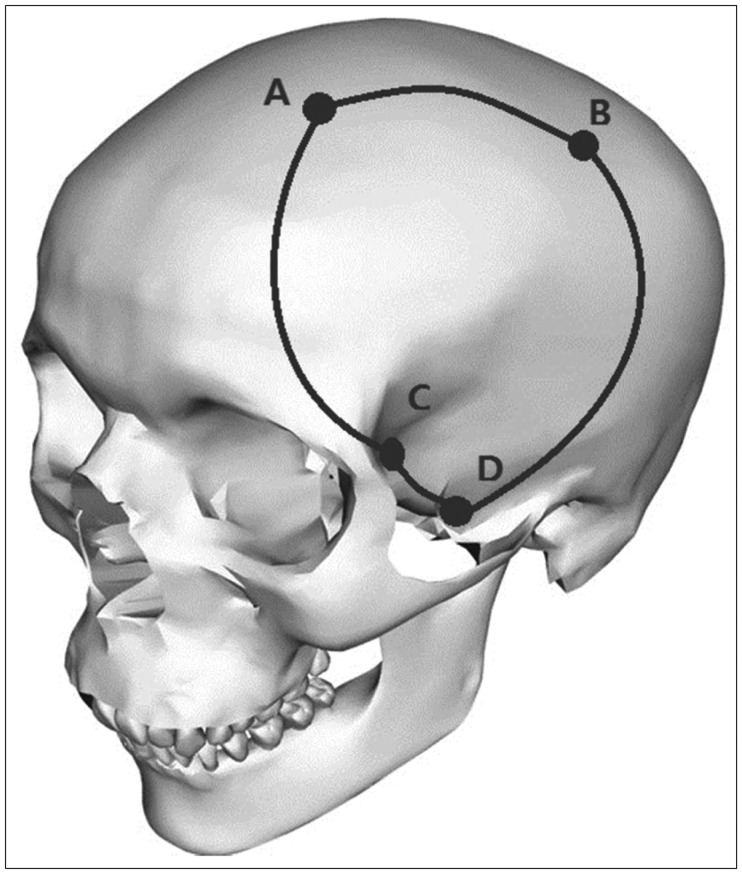 | FIGURE 2Unilateral frontotemporoparietal craniectomy: (A) Frontal area 2 cm in front of the coronal suture and close to the skin incision, (B) Parietal area just posterior to the parietal bone and close to the skin incision, (C) Temporal squama, (D) Key hole area behind the zygomatic arch of the frontal bone.
|
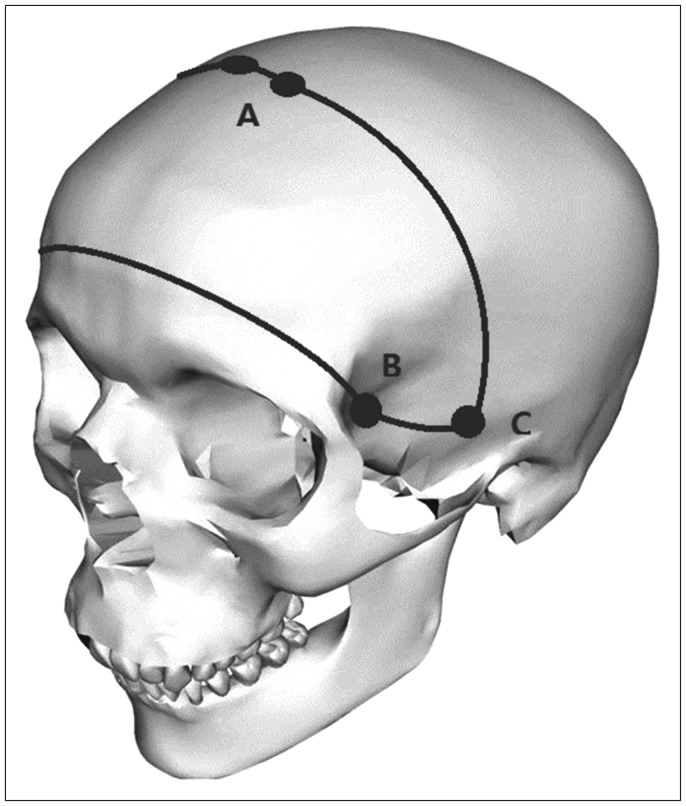
Bifrontal craniectomy allows for frontal contusion of the brain and useful in the cases of generalized cerebral edema without localized lesion. The patient is placed supine position without head rotation and incision begin anterior to the tragus on each side and curve cranially 2 to 3 cm posterior to the coronal suture.43) Careful should be taken not to damage to STA. The incision is taken down through the galea and temporalis muscle to bone. The scalp and muscle flap reflected forward over the orbital rim and expose both supraorbital nerve. Care should be taken not to damage these nerves and dissect out the supraorbital nerve from the supraorbital notch on either side. If the supraorbital notch is closed, only small osteotome can be made to open it. So unfixed supraorbital nerve allow further advancement of the musculocutaneous flap. Burr holes are made in the following areas; 1) Both key hole areas behind the zygomatic arch of the frontal bone, 2) Both squamous parts of the temporal bones, 3) Two burr holes just behind the coronal suture, 1cm apart from midline on each side (Figure 3).43) The SSS can be dissected away from the bone flap by passing Penfield 3 between the burr holes and craniotomy over the SSS should be performed with last cut. After bone flap elevation, bleeding from SSS can be controlled with hemostatic agents including Gelfoam or Surgicel covered with the cottonoid. The key point to durotomy with a bifrontal craniectomy is dividing the anterior portion of SSS and underlying falx. To cross the anterior part of SSS, ligation of the most anterior part of the SSS with two heavy sutures and cut were necessary. Otherwise, the brain does not expand enough and can be damaged by herniation against a tight dural edge.
Go to :
Rationale of DC
The rationale of DC is based in the Monro-Kellie Doctrine. If pathologic conditions that increase ICP is happened, compensatory mechanisms operate to keep ICP constantly. There is exponential relationship between intracranial volume and ICP.47) The abrupt deterioration of altered mentality after TBI could be explained with that relationship.
The skull is a rigid unexpandable structure, opening the cranial vault by DC increases the volume available to the intracranial contents and reduces ICP. Evacuation of hematoma also attribute to reduction of ICP.56)
Two major factors that lead to elevated ICP are mechanical and vascular effect. When a mass lesion develops, a pressure gradient occurs, that cause displacement of the brain tissue and inducing brain herniation. Herniation should be treated immediately to prevent irreversible and fatal damage to the brain stem. Vascular effects of increased ICP are caused by reduced CPP, which is caused by decreased mean arterial pressure (MAP) or increased ICP. As the CPP decreases, CBF may become insufficient for adequate brain-tissue perfusion and oxygenation.1941) Ischemia will induce further cytotoxic edema and result in even higher ICP. A CPP less than 60 to 70 mmHg is associated with diminished oxygenation and altered metabolism in brain parenchyme.30) It is clear that patients with untreated intracerebral hemorrhage (ICH) (ICP ≥20 mmHg) after TBI will result poor outcomes, and improved ICP correlates with improved functional outcome.467) Current Brain Trauma Foundation guidelines suggested the ICP lower than 20 to 25 mmHg after TBI.16) Patients with well-controlled ICP under the threshold appear to have improved outcomes.45) The treatment of increased ICP is very important for the prognosis of patients. Initial managements used such as analgesia, sedation, elevation of the head, CSF drainage through a ventricular catheter (if present), and optimization of ventilation to maintain normal arterial partial pressure of carbon dioxide. Tier therapies are followed as intravenous administration of hyperosmolar solutions, neuromuscular blocking agents, hypothermia, and barbiturate coma therapy.
Go to :
Complications of DC
Although DC is an effective treatment in TBI, there is more than 50% chance of complication related to this.27) One of the risk factors for complications are age and initial neurologic state (lower GCS).45) Risk factors for infection rate is related to invasion of orbital roof during DC, proximity to facial sinuses, and large contour abnormalities with corresponding large dead spaces.1) Potential complications of DC include CSF absorption disorder (subdural hygroma and hydrocephalus), postoperative hematoma expansion, syndrome of the trephined and surgical site infection. Subsequent cranioplasty has the risk of infection, cerebral edema and bone flap reabsorption.
Expansion of hematoma
The expansion of hematoma is the most common and fatal complication in patients who have had a DC after TBI. Due to the dynamic process of TBI, new lesion or existing hematomas can expand after surgery, especially in patients with disseminated intravascular coagulopathy (DIC) or platelet dysfunction due to severe bleeding previously. This phenomenon explains the tamponading effects of increased ICP and cerebral edema has been eliminated and new or in situ hematoma can be recurred. Contralateral hematoma after DC occurs up to 7.4%, so postoperative computed tomography (CT) scan is mandatory because they appear early after surgery.245)
CSF related complications
Subdural hygroma is common complication after DC and occured due to an unbalance between production and reabsorption of CSF. The theory is ruptured arachnoid creating a one-way valve for CSF flow, pressure gradients between hemispheres due to reduction of ICP and decompression of one hemisphere, and alterations in the brain's shape, when performing the DC. Performing duroplasty during DC the incidence of hygroma can be reduced. It is uncommon present worsening clinical symptoms related to hygroma and most of them are reabsorbed spontaneously, but when its expansion aggravate neurological symptoms surgical treatment should be considered.45) Development of hydrocephalus after DC is in up to 2% to 30% of cases, and can complicate the prognosis. Its appearance may be associated with the alterations in the circulation of the CSF. It is usually improved after cranioplasty, but it can persist for a long time despite the replacement. Sometimes, placement of a ventriculo-peritoneal (V-P) shunt is required. The indications of V-P shunt are; the lumbar CSF pressure is consistently >180 mmH2O, the typical symptoms of normal pressure hydrocephalus are present, unless there are surgical contraindications.55) The major complication related to CSF is CSF leakage which can lead to wound complications, infection and prolongation of recovery. A simple CSF leak should be treated with tightening suture of the wound and ventriculostomy initially. If leakage continue, shunting operation should be performed.
Wound problems
The problem related to cutaneous healing has an incidence of up to 10%. The urgent surgical procedure of DC can damage the STA, and reduce flow to the scalp flap that may cause necrosis of the surrounding tissue. Accidentally open the frontal sinus especially bifrontal craniectomy can contaminate the surgical field. The wound infection decreases its incidence due to the administration of antibiotics during surgery, which remains at around 7%. Moreover, the tight sealing of the dura prevents CSF leaks can reduce CSF leakage related wound problems.
Syndrome of the trephined
Its clinical symptoms are headache, dizziness, irritability, seizure, discomfort and psychiatric symptoms especially related to large cranial defects.255) The mechanism explaining this syndrome is not clear, but has been associated with CSF flow abnormalities, direct atmospheric pressure on the brain, and disturbances in CBF. Performing early cranioplasty before the skin flap sink can reduce the syndrome, but it may increase the risk of infection and thus is not recommended.55)
Go to :
Recent Clinical Studies in DC
DC in diffuse TBI (DECRA)
The DECRA trial published by Cooper et al.9) in 2011, is the famous RCT to determine the therapeutic effect of DC in TBI. During 2002 to 2010, 155 patients who had TBI and either GCS score lower than 8 or CT demonstrating moderate diffuse brain injury were enrolled. Patients with refractory ICP (ICP>20 mmHg for 15 minutes within a 1-hour period) were randomized to two group and 72 patients performed DC plus maximal medical care and 82 patients had maximal medical management including barbiturate and hypothermia. The conclusion of this study is DC decrease ICP and the length of stay in the intensive care unit, but is associated with more unfavorable outcomes.9) Interpretations of ICP-related results from DECRA have ranged from arguments that ICP reduction may not necessarily result in better outcomes, to criticism of DECRA study design suggesting that a higher ICP threshold be used for performing DC in TBI.2148) The reason of worsening in DC group are the followings; surgical complication (37%), axonal stretch, aggravated brain edema that would otherwise have been self-limiting. There are some comments and criticisms about the result of DECRA trial.312224650) First, the randomization of patients group was uneven. More patients who had non-reactive pupil were enrolled in the DC group (27%) on the other hand 12% in medical therapy group. If it adjusted the unfavorable outcome showed no difference between two groups. Second, the enrolled patients could not represent the entire real world. Third, in choice of surgical method, only bifrontal DC without falx sectioning was allowed in DECRA trial and it result the advantages of surgical treatment were not prominent. Fourth, the definition of refractory ICP in this trial was too low in pressure and too short in duration. It could not be sure it really reflect intractable increased ICP. Moreover, no standardized rehabilitation, long enrollment period, less concern of CPP are the weak point of this trial.
Trial of DC for traumatic intracranial hypertension (RESCUEicp)
Although the DECRA trial was reported, the effect of DC in TBI patients were remains unclear. Hutchinson el al.23) in 2016 reported multicenter (48 center, 19 countries) RCT study named RESCUEicp. For 10 years from 2004, 408 patients (age, 10-65 years) with TBI and refractory elevated ICP (>25 mmHg) were randomized to undergo DC or receive ongoing medical care. Patients with bilateral dilated pupils, bleeding diathesis, devastating injury, brain stem damage and impossible for follow up were excluded. The primary outcome was the rating on the Extended Glasgow Outcome Scale (GOS-E) at 6 months. At 6 months, the patients in DC group resulted in lower mortality and higher rates of vegetative state, lower severe disability and upper severe disability than ongoing medical care group. The rates of moderate disability and good recovery were similar in the two groups. The result of this trial showed different outcome in contrast to the DECRA trial. Differences between the two trials are summarized in Table 1. The reasons for this is thought to arise from the following differences. The DECRA trial aimed to assess the effectiveness of early DC (within 72 hours after trauma) in moderate ICH (ICP>20 mmHg for 15 minutes within a 1-hour period).9) On the other hand, the aim of RESCUEicp trial is assess the effectiveness of DC in a last-stage treatment with refractory ICH (ICP>25 mmHg for lasting more than 1-12 hours). Moreover, patients with intracranial hematoma were not included in DECRA trial, but in RESCUEicp trial, the patients with intracranial hematoma accounted for almost 20% of cases. The difference of two trials in protocol of surgical method is unilateral hemicraniectomy was not permitted in DECRA trial contrary in RESCUEicp trial. This study supports the debates of previous hypothesis that DC simply increases the number of patients surviving in a vegetative state.34) The survival advantage of DC in this trial was translated to both dependent and independent living. Clinicians and family members will need to be aware of this issue when making decisions regarding treatment options. There are some limitations in RESCUEicp trial. First, the clinical teams who cared for the patients were aware of trial-group assignments. Second, a relatively large proportion of patients in the medical group underwent DC. Third, 10 patients were excluded from all analyses owing to withdrawal of consent or to a lack of valid consent, and seven more patients in the medical group were lost to primary follow-up. Fourth, long-term data on cranial reconstruction were not systematically obtained owing to the pragmatic nature of the trial. Finally, the present trial did not examine the effectiveness of primary DC, which is undertaken more frequently than secondary surgery.
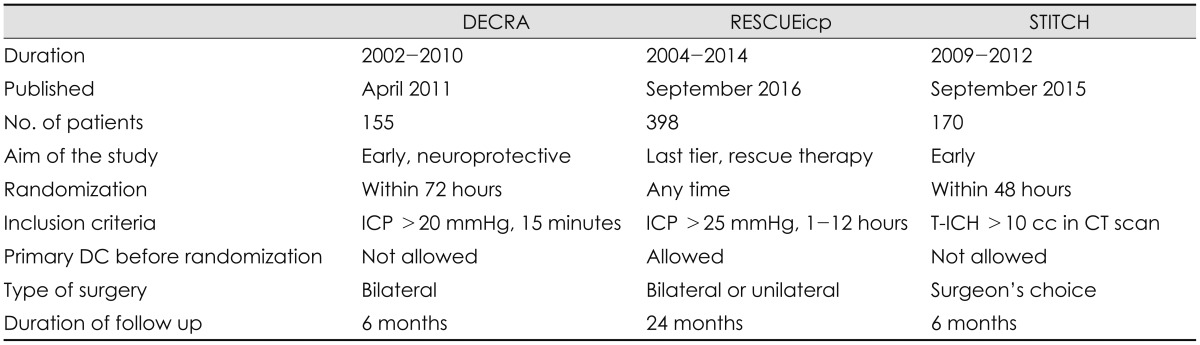
TABLE 1
Differences between the randomized controlled trials for decompressive craniectomy in traumatic brain injury
DECRA: decompressive craniectomy, RESCUEicp: randomised evaluation of surgery with craniectomy for uncontrollable elevation of intracranial pressure, STITCH: surgical trial in traumatic intracerebral hemorrhage, DC: decompressive craniectomy, ICP: intracranial pressure, ICH: intracerebral hemorrhage, CT: computed tomography
![]()
Surgical trial in traumatic ICH (STITCH)
The STITCH Trauma Trial is assessing whether surgery makes a difference for patients with traumatic ICH and contusion. Mendelow et al.39) in 2015, reported international multicenter, patient-randomized, parallel-group trial compared early surgery (hematoma evacuation within 12 hour of randomization) with initial conservative treatment (subsequent evacuation allowed if deemed necessary). Patients who enrolled in this trial were randomized within 48 hour of TBI. Patients who had more than two intraparenchymal hemorrhage of 10 cc or more and have an EDH or SDH that need surgery were excluded in this trial. The treatment outcomes were obtained by postal questionnaires after 6 months. Patients were randomized to early surgery group and 85 patients were in initial conservative group. The treatment outcome were 30 of 82 patients in early surgery group (37%) had an unfavorable outcome and 40 of 85 patients in initial conservative group (47%) had an unfavorable outcome with an absolute benefit of 10.5%. The result showed significant more deaths in the first 6 months in the initial conservative treatment group (p=0.006).
Go to :
Conclusion
Although more research is needed, DC is one of the available treatments for patients with TBI. Especially in the cases presence of intracranial hematoma was more useful than in cases of diffuse brain edema. It showed better outcome to perform the operation early after the injury. However, in patients with severe 361 damage, the survival rate was increased by DC, but the severe disability including vegetative state was not prevented.
Go to :
 XML Download
XML Download