

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Acute subdural hematomas (ASDH) are observed in one third of patients with severe traumatic brain injury.22) ASDH forms between the dura and arachnoid membranes usually due to tearing of bridging veins or arterial rupture. Management of ASDH may vary from simple observation to different surgical evacuation technique. Two most frequent surgical modalities are craniotomy (CO) and decompressive craniectomy (DC). CO procedure removes skull bone and subdural hematoma followed by replacement of original skull bone. DC also removes skull bone and hematoma, but remains the bone unclosed for possible expansion of edematous brain tissue with or without an additional expansile duroplasty.2)
Many studies have been reported showing effectiveness of DC for ASDH.156101718) However, not all patients show severe postoperative brain swelling after evacuation of hematoma where theoretical benefit of DC is questionable. DC also carries disadvantage owing to lack of bone closure.291016) The optimal surgical modality for ASDH still remains to be clarified.
The objective of this study is to analyze the surgical outcomes of CO and DC for evacuation of ASDH by comparing the preoperative clinical features, computed tomography (CT) images and postoperative complications which may possibly aid in selection of optimal surgical modality.
Go to : 
Materials and Methods
We retrospectively reviewed 46 cases of ASDH surgically treated with CO or DC in our hospital from January 2010 to December 2014. Demographic and preoperative medical data were reviewed including age, sex, and presence of medical illness causing coagulopathy or use of antiplatelet agents. Preoperative data that may affect the surgical outcome were also collected such as time from trauma to surgery or time from clinical deterioration to surgery, preoperative Glasgow Coma Scale (GCS), pupillary light reflex, and presence of major extracranial injury. Preoperative CT scans were analyzed for measurement of midline shift, presence of intracerebral hemorrhage (ICH) or petechial hemorrhage, obliteration of basal cistern and third ventricle, and presence of subarachnoid hemorrhage at basal cistern.
All of the patients underwent surgery for evacuation of ASDH through frontotemporoparietal CO of size 10×12 cm or larger. Decision for CO or DC was done by attending neurosurgeon (Figure 1). Cases in which evacuation ASDH were not the main goal of surgery were excluded. Thus, evacuation of large traumatic ICH, decompression for cerebral swelling, and surgery other than frontotemporoparietal CO were excluded in this study.
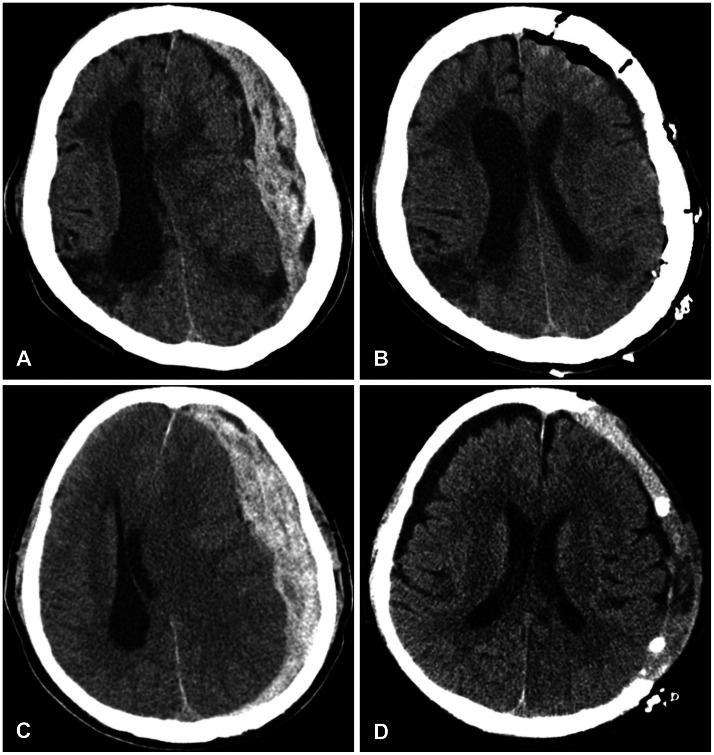 | FIGURE 1Preoperative (A) and postoperative (B) computed tomography (CT) scan of 75-year-old female with acute subdural hematomas (ASDH) after traumatic brain injury. She underwent craniotomy and evacuation of hematoma without remarkable postoperative brain swelling. Another case of 78-year-old male with ASDH (C, D) who underwent decompressive craniectomy. Preoperative (C) and postoperative (D) CT scan shows brain swelling, but removal of bone aids in control of raised intracranial pressure.
|
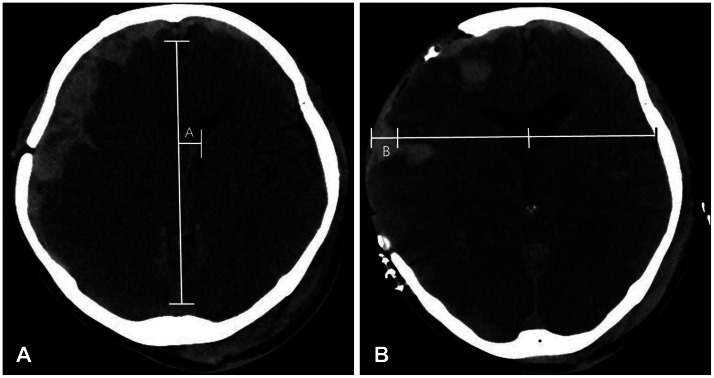
Postoperative midline shift was measured from immediate postoperative CT scan. Measurement of swelling above the bone flap was done for patients who underwent DC with CT scan taken within postoperative day 3 to 7 when maximal brain swelling was observed. Imaginary line on absent bone flap was drawn and brain tissue above the imaginary line was measured (Figure 2). Medical records and CT scans were reviewed for patient who underwent cranioplasty. Postoperative outcome was recorded using modified Rankin Scale (mRS) 6 months after initial surgery. Outcome was defined good for patients with mRS score 1-3, and poor for patients with scores 4-6.
Preoperative clinical features were classified for further analysis where unfavorable feature was defined as age over 70 years, anticoagulation or antiplatelet use, time to surgery >4 hours, preoperative GCS <8, one or both non-reactive pupil, and comorbid major extra-cranial injury. Preoperative CT findings with ICH or petechial hemorrhage, obliterated basal cistern or 3rd ventricle, and presence of subarachnoid hemorrhage were also classified as unfavorable preoperative feature.
Data was analyzed using Statistical Package for Social Sciences (SPSS) software for personal computers (SPSS ver. 21; IBM Corp., Armonk, NY, USA). Unpaired Student's t-test or Mann-Whitney test was used for continuous variables, and chi-squared test or Fisher's exact test was used for categorical variables. Probability value of less than 0.05 was considered as statistically significant.
Go to :
Results
Demographic and preoperative clinical factors
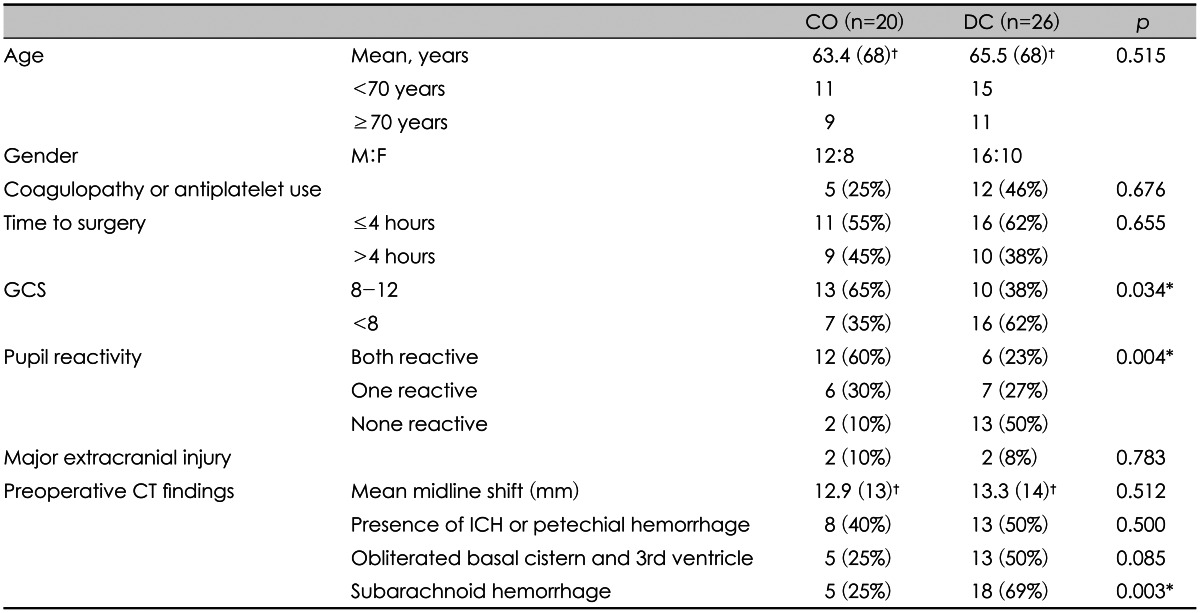
Forty six patients met the inclusion criteria of patient with ASDH who received either CO or DC. Twenty (43%) patients underwent CO, and 26 (57%) with DC. Mean age of CO group was 63.4 years, and DC was 65.5 years. Male was prevalent in both groups. Neither age nor gender distribution showed significant difference between the groups.
Preoperative clinical data showed presence of coagulopathy or use of antiplatelet in 5 of 20 (25%) patients of CO group and 12 of 26 (46%) patients of DC group. Time to surgery or clinical deterioration to surgery time was less than 4 hours in 11 of 20 (55%) patients in CO group and 16 of 26 (62%) patients in DC group. No statistical difference between the two groups was significant in above preoperative clinical features. However, more patient in DC group had preoperative GCS <8 (35% in CO vs. 62% in DC, p=0.034). Preoperative pupillary reflex also showed more one or both non-reactive pupil in DC group (40% in CO vs. 77% in DC, p=0.004). Major combined extracranial injury were 2 patients in both groups (Table 1).
Preoperative CT findings
Mean preoperative midline shift at preoperative CT were 12.9 mm in CO group and 13.3 mm in DC group (p=0.512). Number of patients with ICH or petechial hemorrhage was 8 in CO group and 13 in DC group (40% in CO vs. 50% in DC, p=0.500). Obliteration of basal cistern and 3rd ventricle was 5 in CO group and 13 in DC group (25% in CO vs. 50% in DC, p=0.085). More patients showed preoperative subarachnoid hemorrhage in DC group (25% in CO vs. 69% in DC, p=0.003).
Postoperative findings and patient outcome
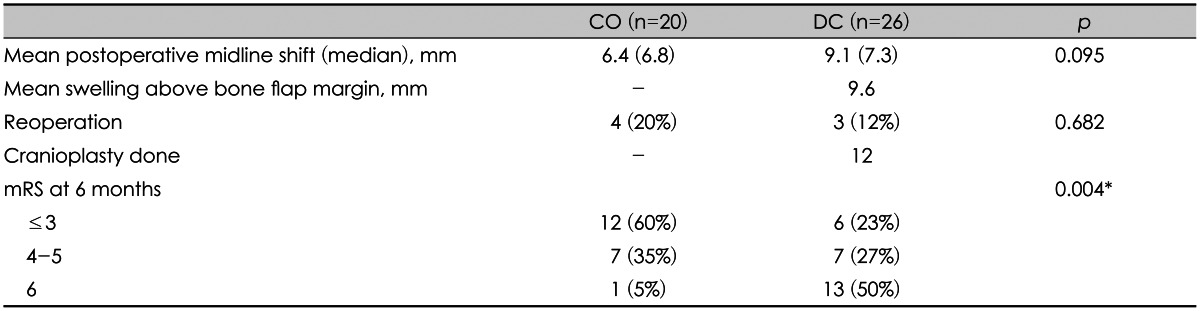
Mean postoperative midline shift was larger in DC group (6.4 mm in CO vs. 9.1 mm in DC), but it was not statistically significant (p=0.095). Reoperation was done in 4 of 20 (20%) patients in CO group which were due to recollection of subdural hematoma in 2 patients and epidural hemorrhage in 2 patients. In DC group, reoperation was done in 3 of 26 (12%) patients which were due to subgaleal hematoma in 1 patient and growth of traumatic ICH in 2 patients. Cranioplasty was done in only 12 of 26 (46%) patients mainly due to patient condition. Six months postoperative mRS scores were less than 3 in 12 (60%), 4 & 5 in 7 (35%), and 6 in 1 (5%) of 20 patients in CO group. In DC group, mRS scores were less than 3 in 6 (23%), 4 & 5 in 7 (27%), and 6 in 13 (50%) of 26 patients. Difference of 6 months mRS scores between CO and DC groups were statistically significant (p=0.004) (Table 2).
Number of unfavorable preoperative features and clinical outcome
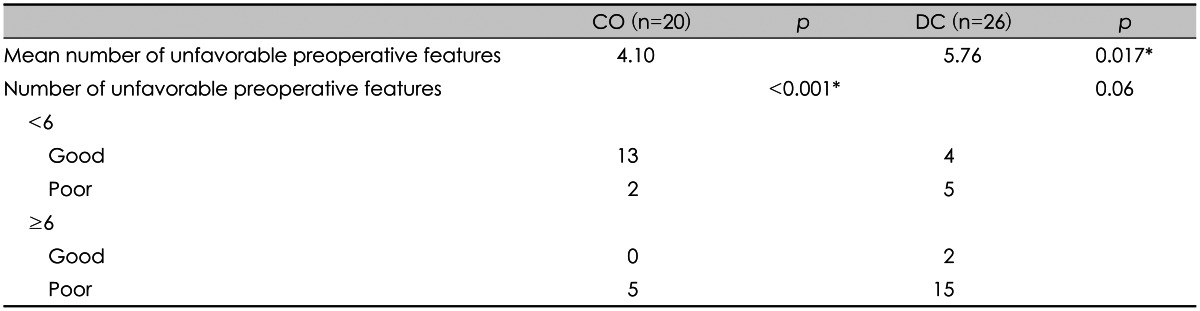
Mean number of unfavorable preoperative feature was 4.1 in CO group, and 5.8 in DC group (p=0.017) (Table 3). In CO group, patient with preoperative adverse feature <6 showed good outcome in 13 patients and poor in 2 patients. With preoperative adverse feature ≥6, no patient showed good outcome and 5 patients showed poor outcome (p<0.001). In DC group, patient with preoperative adverse feature <6 showed good outcome in 4 patients and poor in 5 patients. With preoperative adverse feature ≥6, 2 patient showed good outcome and 15 patients showed poor outcome (p=0.06).
Go to :
Discussion
ASDH are present in approximately one third of patients with severe traumatic brain injury.22) Despite advances in emergency medical services and surgical techniques, ASDH remains one of the most lethal of all intracranial injuries. Various surgical modality such as simple burr hole trephination, CO, and DC are used for evacuation of ASDH. On the Brain Trauma Foundation guidelines published in 2006, they recommended that ASDH with thickness greater than 10 mm, or midline shifting greater than 5 mm on CT scan should be treated surgically.1) Mortality rates of ASDH ranges from 55% to 79% even with surgical intervention of any modality.19)
Ransohoff et al.18) reported recovery rate of 40% for ASDH treated with hemicraniectomy followed by hematoma removal. After the report, DC for ASDH has been recommended as a surgical modality of choice, and performing DC in ASDH patients seemed to be attractive.1478131420) Girotto et al.7) reported DC technique of adequate size, early surgery, and GCS of 6 to 8 group would contribute significantly to better outcome by reducing morbidity and mortality. Meier and Gräwe17) reported that DC benefits on overall outcome of patients with traumatic brain injury. The rationale behind performing DC lies in control of postoperative brain swelling and overwhelming intracranial hypertension, but little is known on the degree of postoperative swelling after evacuation of hematoma. Empirical decision for DC or CO is made by the neurosurgeon based on patients' clinical status and CT findings which may be confounding unless brain swelling is noted intraoperatively after evacuation of hematoma.
The analysis of postoperative brain swelling is difficult since the postoperative CT findings or intracranial pressure measurements will vary depending on closure or opening bone flap. Different trauma setting among patients makes randomized trial for CO and DC impossible and unethical. Nevertheless, there were several retrospective series that compared the outcome of CO and DC.35121521) Woertgen et al.21) compared the surgical outcomes in ASDH which were not significantly different between CO and DC. They concluded that signs of herniation at presentation, and increasing age had most influence to patient outcome. So, preoperative clinical feature influenced most on outcome and DC does not seem to have a therapeutic advantage over CO in ASDH. More recent study by Chen et al.3) also reported similar results in 102 patients where DC group had higher mortality rate which may be due to poorer preoperative clinical status. The study by Li et al.15) is notable where they tried to diminish the effect of preoperative clinical status by using CRASH-CT prognostic model. Predicted outcome was calculated in 85 patients in a retrospective fashion. Favorable outcomes were observed in 45% of CO versus 42% of DC (p=0.83), but standardized morbidity ratio (observed/expected unfavorable outcome) was 0.90 for CO group and 0.75 for DC group.
Our study showed poorer outcome in DC group compared with CO group (poor mRS 77%, 20 of 26 patients in DC group vs. 40%, 8 of 20 patients in CO group; p=0.004). This results are may be due to more patients with low GCS score (GCS<8), unresponsive pupil, and comorbid CT lesion in DC group. Our results carry similar selection bias that neurosurgeons tend to perform DC when patients' preoperative clinical status is poor. To clarify this point, we counted on number of unfavorable features for each patient that may influence on poor outcome. On average, DC group had more adverse features than CO group, and thus poor outcome for DC group can be explained.
One notable finding is that in patients with few unfavorable features (<6), good outcome (mRS less than 3) was achieved in majority of patients in CO group. However, similar results were not obtained in DC group with few unfavorable features. This implies that further stratification of unfavorable clinical features is needed which has larger impact on outcome. Nonetheless, it seems that some patients with few preoperative unfavorable features can benefit with CO without the need for bone removal.
Furthermore, various possible complications of DC need awareness of neurosurgeons. Subgaleal hemorrhage, herniation through the cranial defect, subdural effusion, syndrome of the trephined (sinking skin flap syndrome), and hydrocephalus were reported complications of DC.1123) In our series, 1 patient underwent reoperation due to subgaleal hematoma and 2 patients had severe sinking of skin flap where difficulty was in cranioplasty resulted in complication. DC also have disadvantage of requiring subsequent cranioplasty which harbor additional risk of complication.21116) Gooch et al.9) reported that immediate post-operative complication rate of cranioplasty after DC was as high as 34% which were infection, wound breakdown, intracranial hemorrhage, and bone resorption. We also experienced complications of cranioplasty in our patients (4 of 12; epidural hematoma 2, infection 1, cerebrospinal fluid leakage 1) which interrupted patients' recovery. In this context, there may be some advantage of CO in evacuation of ASDH.
However, this study is a retrospective single center study with small patient population. Limitations of selection bias hinder any conclusion on role of CO or DC for ASDH. We think further investigation with larger patient population and carefully selected criteria is needed to clarify the optimal surgical modality for patient with ASDH.
Go to :
Conclusion
In selective cases of few unfavorable clinical findings, CO may also be an effective surgical option for ASDH. Although DC remains to be standard of surgical modality for patients with poor clinical status, CO can be an alternative considering the possible complications of DC. Controlled prospective study with larger patient population is needed clarify this point.
Go to :
 XML Download
XML Download