

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Retro-odontoid pseudotumor (ROP) or pannus is a non-neoplastic mass at the craniovertebral junction,813) which can cause cord compression and neurological symptoms.28) In most of cases, ROP is associated with atlantoaxial subluxation (AAS) in patients with rheumatoid arthritis (RA).8121314) However, ROP has been rarely reported in patients without RA and ASS.13) The exact mechanism of ROP formation without AAS and RA is unclear. Here, we report a rare case of ROP developed in patients without both RA and AAS and suggest a possible mechanism with literature review.
Go to : 
Case Report
A 76-year-old woman presented with progressive gait disturbance and dysesthesia at posterior neck for 3 weeks. The patient had no history of RA. Neurological examination revealed typical cervical myelopathy with clumsiness of both hands, gait disturbance and hypesthesia on both extremities. In laboratory study, serum rheumatoid factor and anti-cyclic citrullinated peptide antibody were negative. A physical examination showed no signs of RA, such as polyarthritis of the hands, wrist, and feet and extraarticular disease manifestation. Dynamic radiography of the cervical spine showed no evidence of AAS, showing only 2 mm of atlantodental interval (Figure 1). Magnetic resonance image (MRI) showed a retro-odontoid mass extending from posterior part of axis up to cranial base, and compressing the spinal cord. The mass was seen as an iso-intensity area on T1-weighted images (WI), a mixture of low- and high-intensity on T2-WI, with absence of contrast enhancement after gadolinium administration. The T2-WI showed a high-intensity area in the intramedullary region of the upper cervical spinal cord (Figure 2). Computed tomography (CT) showed no calcification in the mass and severe spondylotic change with facet joint osteoarthritis at whole cervical spinal segments (Figure 3). Based on the radiographical findings, the differential diagnosis was ROP. However, because the patient had no RA and AAS, the tumorous lesions or disc herniation should be considered as a differential diagnosis. Considering her old age and no AAS, we planned mass removal and biopsy only via a minimal laminectomy. First, left lateral suboccipital craniotomy and hemilaminectomy of C1 were performed, but the mass was not exposed by extradural view. Thus, transdural approach was tried to remove the mass. Paramedian durotomy was performed and ventral dura also opened beside the spinal cord and rootlets. After opening of ventral dura, yellowish fluid was expelled and yellowish friable mass was easily removed by a ring curette. Enough decompression was performed and ventral and dorsal dura was closed water-tightly. Further C1-2 fixation was not performed. Postoperative CT showed subtotal removal of the mass (Figure 4A). Histopathological examination confirmed the lesion as a pannus with degenerative cartilage. Postoperatively, her symptoms were slightly improved, but again aggravated 2 months after surgery. Dynamic X-rays showed newly-onset AAS showing 5 mm of atlantodental interval. A follow-up MRI showed the re-grown mass, but still spinal cord compression due to the mass and AAS (Figure 4B). Based on histopathological diagnosis of pannus, a posterior C1 lateral mass-C2 pedicle screw fixation was performed without further mass removal or laminectomy. From 3rd postoperative day, she showed marked improvement of the symptom. Twelve months after the operation, a follow-up MRI showed complete resolution of the ROP with C1-2 bony fusion and her symptoms completely improved (Figure 4C).
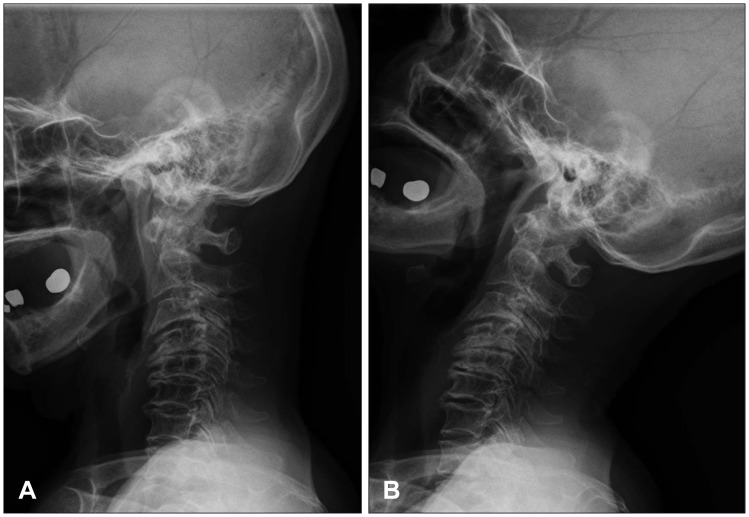 | FIGURE 1Dynamic flexion cervical radiographs (A) and extension (B) showing no evidence of atlantoaxial subluxation.
|
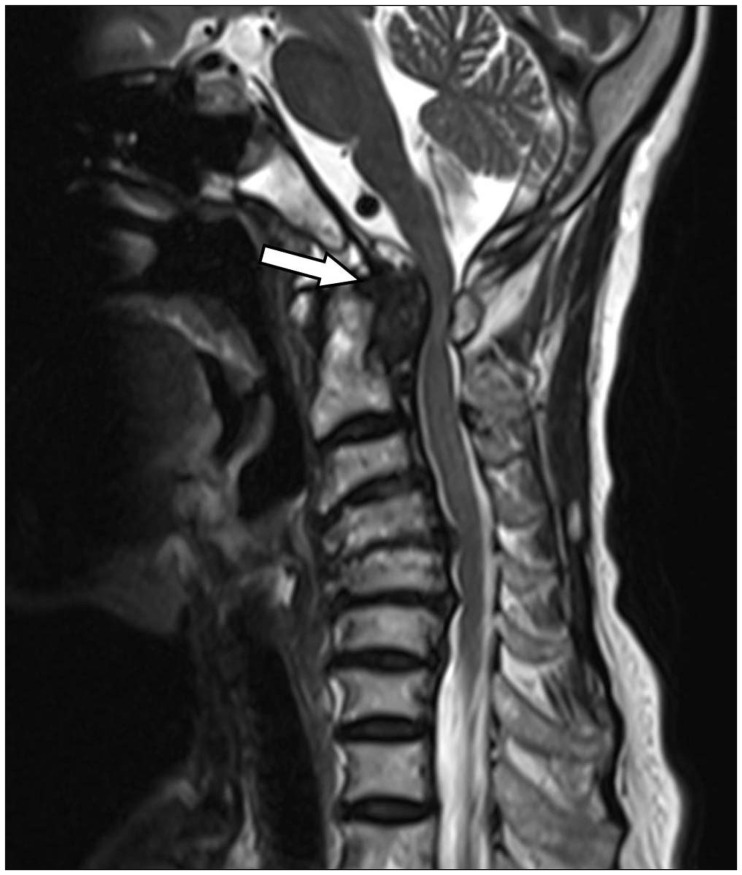 | FIGURE 2A magnetic resonance imaging showing retro-odontoid pannus compressing the spinal cord, that appears as an area of mixed intensity on sagittal T2-weighted image (arrow).
|
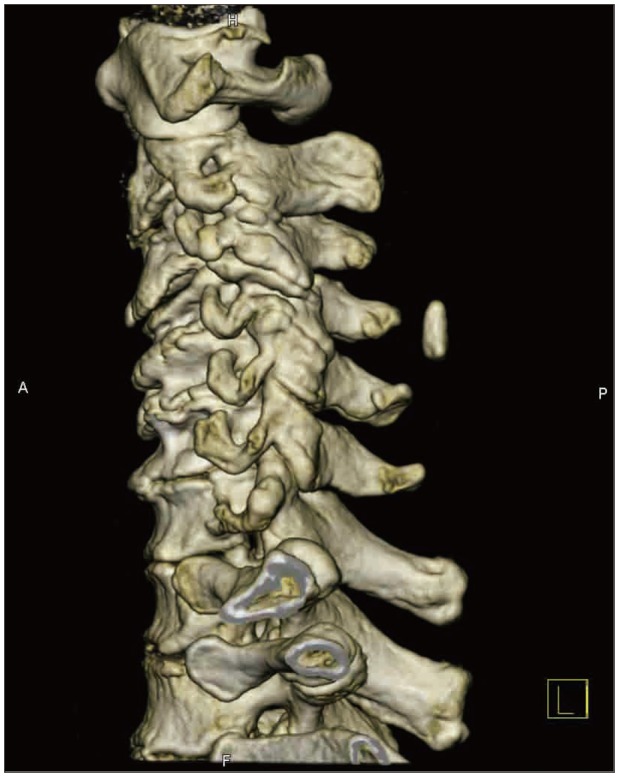 | FIGURE 3A 3-dimention cervical computed tomography scan showing spondylotic change of whole cervical spine.
|
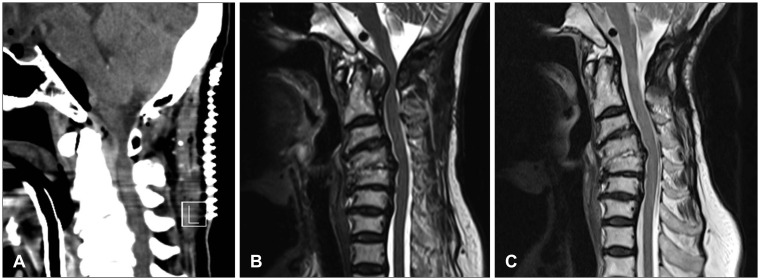 | FIGURE 4Postoperative cervical spine computed tomography showing hemilaminectomy of C1 and debulked the retro-odontoid mass (A). Postoperative (2 months later) magnetic resonance imaging (MRI) showing remnant retro-odontoid mass (B). After posterior C1-2 fixation surgery, follow magnetic resonance imaging (C) showing no evidence of retro-odontoid mass.
|
Go to :
Discussion
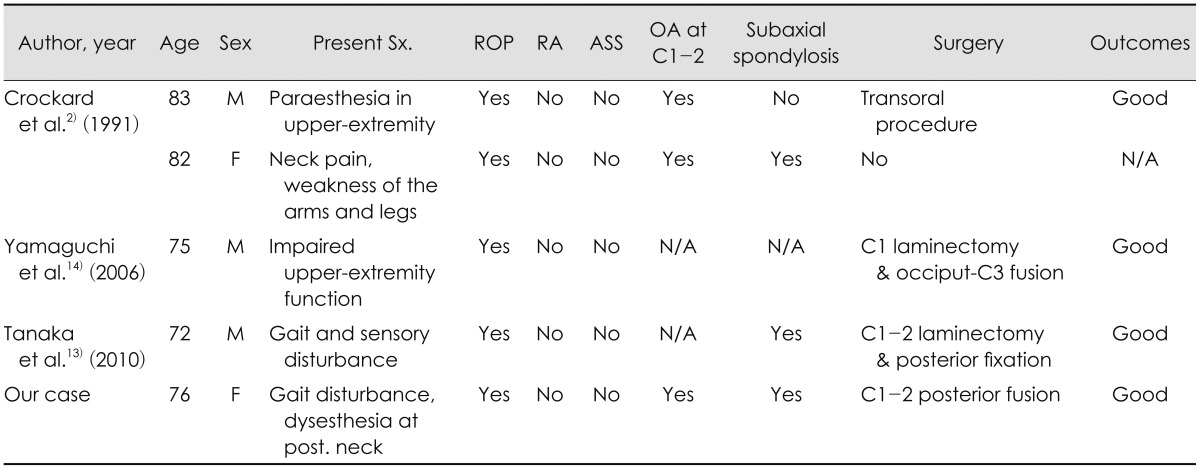
ROP is frequently associated with RA.38121314) In RA, the pannus formation is attributed to inflammation of the synovial membrane, resulting in overgrowth of the hyaline cartilage and peri-articular inflammation.4) Consequentially, inflammation, ligament laxity, and bone erosion result in C1-2 joint laxity and subluxation. Although uncommon, a ROP can be developed due to AAS in patients without RA.13) AAS exerts mechanical stress and injury on the transverse ligament of the atlas, resulting in a reactive hypertrophied mass. Therefore, AAS may play an important role in the development of ROP.61012) However, like our case, a ROP unassociated with both AAS and RA is extremely rare. Only four cases of ROP unassociated with both AAS and RA have been previously reported (Table 1).271314) The exact mechanism of pannus formation is unclear. However, the previous reports suggested that loss of mobility at middle and lower cervical segment, and resultant excessive motion of the C1-2 segment transfer the mechanical stress to the atlantoaxial joint, resulting in pannus formation.1315) In the case, mobility below the C2 cervical spine was limited by spondylosis and facet fusion at C2-3-4 levels. In our case, severe multiple spondylotic change of subaxial cervical spines were also found. However, in the other reports, a ROP developed in patients with mild spondylosis or without spondylosis in subaxial cervical spine.61011) Therefore, only loss of mobility associated with subaxial cervical spondylosis is difficult to completely explain the mechanism of ROP formation in patients without AAS. Reviewing the reported cases and our case, we found two common points in the patients. All patients were more than 70 years old and most had moderate or severe osteoarthritic change at atlantoaxial joint. Thus, we speculated that moderate or severe osteoarthritis of C1-2 itself causes a partial tear or degradation of the transverse ligament. Resultant vicious cycle of repair and injury may lead to progressive ROP. However, unlike RA, the ROP in the elderly may be not associated with overt AAS. Instead, we suggest that stiffness due to severe osteoarthritis of lateral atlantoaxial joints may prevent the overt AAS, offsetting the effect of loose transverse ligament. Nevertheless, we still believe that C1-2 instability play a key role in development or progression of ROP because most of ROP associated with AAS and often resolve spontaneously after C1-2 fusion.5678121314) In the elderly with osteoarthritis, even though C1-2 instability is not "overt AAS" on the radiographs, "micro-instability" may be exist and affect the progression of ROP.
Surgical treatment of ROP can be classified into two modalities: 1) direct excision of the mass and 2) posterior decompression and fusion aiming spontaneous tumor regression.114) Direct excision of the mass can be performed by the transoral approach and epidural or transdural approach by posterior laminectomy.1911) However, The transoral approach is vulnerable to cerebrospinal fluid leakage, postoperative infection and postoperative instability.911) The epidural approach may force retraction of the nerve root and spinal cord and have hemorrhagic risk.11) A posterior transdural approach may decrease the distance needed to reach the ROP and does not require retraction of the spinal cord and nerve root. However, if the mass located in the midline of cervical axis or presented with huge size, the posterior transdural approach is limited used for radical resection due to risk of injuries. In our case, differential diagnosis of tumorous lesion or disc herniation should be necessary due to absence of AAS and RA.613) Therefore, in the first operation, we performed direct mass debulking and biopsy by transdural approach with minimal hemilaminectomy. However, the direct mass excision and hemilaminectomy can unexpectedly new-onset AAS associated with additional ligament injury, resulting in re-growth of ROP and neurological aggravation. Recently, posterior decompression and fusion may be considered as first choice of treatment for ROP with AAS.68121314) In our case, C1 lateral mass-C2 pedicle screw fixation without further laminectomy or mass removal was performed and the ROP regressed completely. Goel and Dange4) reported the immediate postoperative regression of ROP after lateral mass reconstruction in the patient with RA.
Go to :
 XML Download
XML Download