

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The sinking skin flap syndrome (SSFS) is a rare complication that occurs in patients with large cranial defects following a decompressive craniectomy (DC).2) A known cause is local in-folding of the scalp or scarring at the craniectomy site between the overlying skin and dura, which exerts direct pressure on the brain.11) Atmospheric pressure also exerts a force against the concave sinking skin flap and underlying brain tissue, influencing cerebrospinal fluid (CSF) flow.15) There are many different neurologic symptoms of SSFS that usually resolves after cranioplasy.39)
Intracerebral hemorrhagic infarction after cranioplasty is a very rare complication with only 4 reported cases to date.3467) We present the occurrence of acute infarction with hemorrhagic transformation involving left cerebral hemisphere following cranioplasty with SSFS.
Go to : 
Case Report
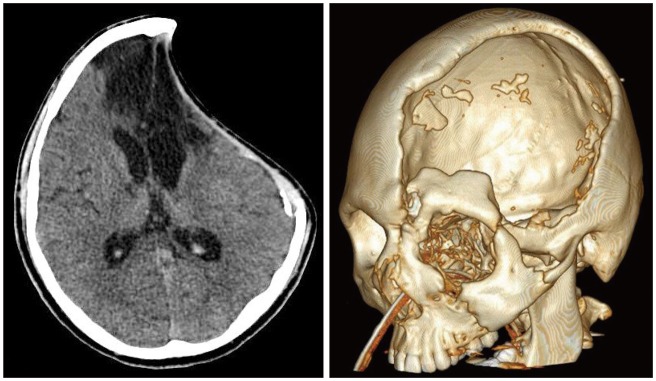
A 20-year-old male biker was brought to the emergency department after being collapsed in the street. The patient had a Glasgow Coma Scale (GCS) score of 9, left eyebrow laceration with sever swelling and 2 mm sluggish right pupil. The patient was stupor and intubated for air way protection. Initial brain computed tomography (CT) revealed epidural and subdural hematoma at left frontotemporal convexity and along the anterior falx with comminuted skull fracture involving left frontotemporal and sphenoid bones (Figure 1). These findings present the high intracranial pressure (ICP). An emergency left frontotemporoparietal DC for hematoma evacuation was performed with duraplasty to treat a brain edema.

At the post operated CT, newly appeared low density lesion involving genu of internal capsule. CT angiography and brain perfusion CT was performed. Left A2 proximal portion was narrowed due to transfalcine herniation to right side and decreased perfusion involving left frontal lobe, [i.e, anterior cerebral artery (ACA) territory] and decreased cerebral blood volume (CBV) & cerebral blood flow (CBF) (Figure 2).
He had suffered from SFSS and fever of unknown origin (FUO) since DC (Figure 3). GCS score was 9 and intermittently partial seizures attack was shown. His face seemed like painful and twisting himself in agony. Laboratory finding and blood culture were within normal limits.
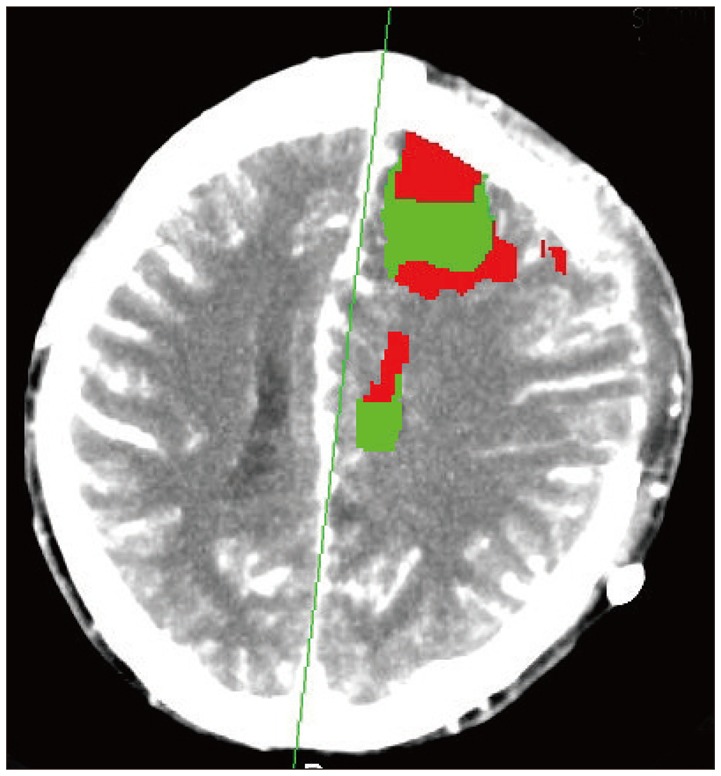
 | FIGURE 3Before cranioplasty brain computed tomography revealed chronic parenchymal defect involving bilateral frontal, left temporal lobes, genu of both internal capsule, both cerebral peduncle and cingulate gyrus. Further decreased brain swelling and associated inward displacement of left frontoparietal dura and skin.
|
After 7 months of craniectomy, cranioplasty was done. Patient stopped seizure and hyperthermia was resolved. He stopped twisting his body and didn't look painful. One day after surgery, he showed a neurologic deterioration. GCS scored 5, heart rate raised upto 130 per minute and scalp swelling occurred. Brain CT, magnetic resonance (MR) image (MRI) and MR angiography (MRA) revealed acute infarction with hemorrhagic transformation involving left cerebral hemisphere (i.e, internal carotid artery (ICA) and posterior cerebral artery (PCA) territory) causing mass effect (Figure 4). No evidence of arterial occlusion or venous thrombosis of intracranial vessels was found on MRA and MR venography (MRV). Heart function was normal.
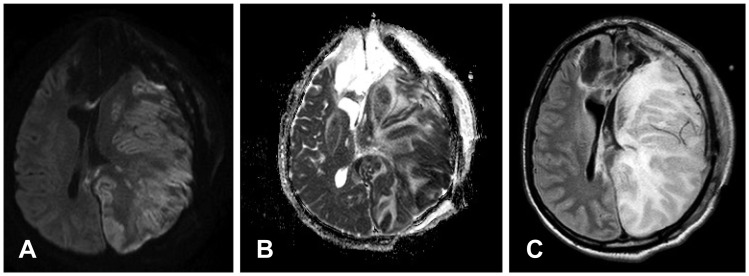 | FIGURE 4After cranioplasty brain magnetic resonance image revealed acute infarction with hemorrhagic transformation involving left cerebral hemisphere (internal carotid artery and posterior cerebral artery territory): Diffuse weighted imaging (A), apparent diffusion coefficient (B) and T2 flair (C).
|
We controlled ICP by using osmotic-diuretics, steroid, and antiepileptic drugs. After 3 days, GCS scored 9, vital sign became stable and neurological symptoms improved. Brain image improved just like after cranioplasty in two weeks later brain CT (Figure 5).

Go to :
Discussion
SSFS is one of complications following large craniectomy and usually manifests as mental state decline, severe headache, seizures or focal deficits after a relatively stable and improved stage. It occurs from several weeks to months after DC.58) After craniectomy, the cranium does not maintain rigid structure. Increased transmission of atmospheric pressure decrease volume of brain and CSF in patients with craniectomy.12)
Transcranial Doppler and 18-fluorodeoxyglucose positron emission tomography shows that cerebrovascular reserve capacity and glucose metabolism improved after cranioplasty.13) Xenon CT and P31 MR spectroscopy (MRS) have shown improved brain perfusion and metabolism after cranioplasty.14) CT perfusion after cranioplasty has demonstrated increase CBF not only in the injured hemisphere but also in the contralateral hemisphere.10)
Hemorrhagic infarction have been reported as a complication of cranioplasty procedure. In our patient, hemorrhagic infarction was involved after cranioplasty, same side of hemisphere. We deem that hemorrhagic infarction is related to the increased CBF on the side of cranioplsty. Rapid increase in bilateral CBF and volume in the chronic dysfunctional brain which lost the ability of autoregulation result in venous stasis and congestion that can lead to thrombosis and diffuse hemorrhagic infarction, and may have increased the risk of hemorrhage.4)
Atmospheric pressure vector on the brain has removed after cranioplasty result in a reexpansion of brain stretch of intracranial vessels. It may induce a transient decrease in perfusion on target tissue as well as microvascular injury, which increases propensity of hemorrhage.3467)
In our case, the patient suffered from SSFS and FUO and it have been resolved after cranioplsty. Therefore, we suggest that FUO maybe one symptom of SSFS.
Go to :
 XML Download
XML Download