

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Intracranial pressure (ICP) control is the main goal in managing traumatic brain injury (TBI). In addition to the direct injury, secondary insult due to post-traumatic increase in ICP or decrease in cerebral perfusion pressure is well recognized as a cause of increased mortality and morbidity.41518222327) Although debates concerning its effectiveness in improving patient outcomes are ongoing, decompressive craniectomy (DC) is widely performed throughout the world to manage TBI.38) Although DC has been shown to decrease ICP,36) there is no clear evidence of an association between DC and better outcomes.32) Therefore, DC is regarded as only an "option" among guidelines for head injury management.24)
Reportedly, acute subdural hematoma (ASDH) is found in up to one third of patients with severe TBI.540) ASDH may be treated conservatively or surgically, and surgery is often undertaken to prevent secondary brain injury upon signs of progressive neurologic deterioration, increased ICP and significant mass effect.5,40) However, many ASDH patients still report unfavorable outcomes.540) For TBI involving ASDH, DC is commonly performed as a salvage procedure for uncontrollable ICP and progressive clinical deterioration despite maximal conservative management.333439) Although DC is generally performed by surgeons to treat TBI, it is still unclear whether early decompression is an optimal treatment strategy for head injury patients with ASDH. However, early DC is performed widely in trauma institutes and is recommended by many studies on the management of TBI.30) Therefore, in this study, we attempted to evaluate the effects of early decompression on ASDH, according to differences in survival outcomes and Glasgow Coma Scale (GCS) score between patients treated with DC early after trauma onset (less than 3 hours between trauma onset and operation) or late after trauma onset (more than 3 hours).
Go to : 
Materials and Methods
A total of 392 patients who underwent DC at single university hospital from April 2002 to March 2012 were retrospectively reviewed after obtaining Institutional Review Board approval. All patients who required DC exhibited a space occupying hemorrhage on computed tomography scan. Among them, patients who underwent DC for ASDH alone or with other cerebral hemorrhages such as traumatic intracerebral hemorrhage, traumatic subarachnoid hemorrhage and intraventricular hemorrhage were included in this study (n=198). Generally accepted indication criteria for DC in this medical university were supratentorial lesion with midline shift on imaging study, altered mental status, pupillary abnormalities, but respond to mannitol and refractory ICP despite best conventional therapy. For each of these patients, we reviewed information recorded by the National 119 Rescue Service together with operation records to assess the length of time between trauma onset and decompression. A total of 65 cases were excluded from this study due to missing data on onset time in 14 cases and a delayed operation (more than 1 day) after closed observation with medical care in 51 cases. Finally, 133 cases of DC with ASDH were included in this study (Figure 1).
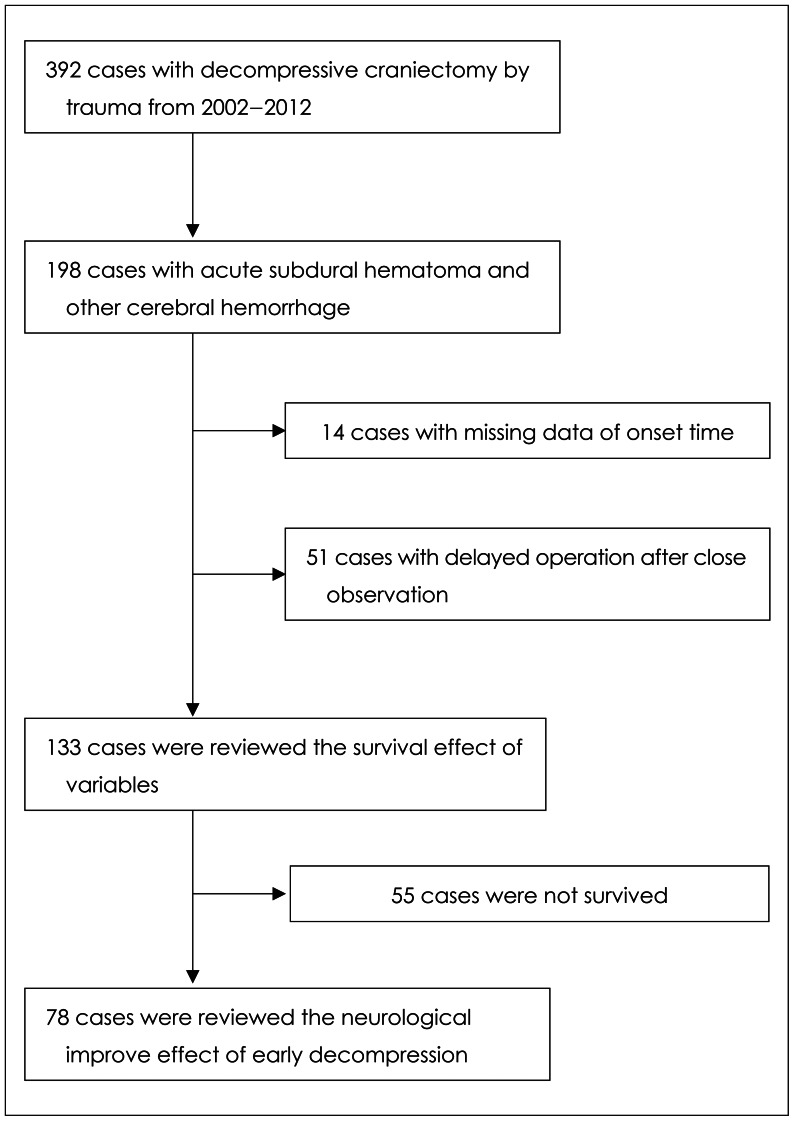
This study attempted to define mortality related factors in DC patients with ASDH. To do so, the variables of sex, age, brain compression ratio, brain stem compression, preoperative mental status, and time interval between trauma onset and operation (the induction time of anesthesia) were assessed in all 133 cases treated with DC for ASDH. Next, we attempted to define the relationships between neurological mental improvement and the time interval between trauma onset and decompression in DC patients with ASDH. Among 133 cases, patients that survived (n=78) were selected and analyzed according to post-operated neurological mental status or improvement (Figure 1).
Neurological outcomes were measured by both the modified Rankin scale (mRS) and according to neurological mental status. The mRS is summarized in Table 1. Neurological mental status was scored according to the GCS (sum of eye opening, verbal response, and motor response). Brain compression ratio was calculated as a shift in the midline over the width of the ASDH at the level of the frontal horn of the lateral ventricle, similar to the brain shifting index of chronic subdural hematomas (Figure 2).1928) Direct pupillary light reflex was evaluated to gauge the compressed level of the oculomotor nerve, as well as the functions of the midbrain and upper brain stem. The pupil diameter was measured using a millimeter ruler, and a fixed pupil was defined as a constriction of less than 1 mm when the light reflex was checked. Based on this definition, brain stem compression was defined as a pupil grade of less than 3, as categorized by Xiao et al.41) Pupil grade was categorized as either Grade 0, bilaterally fixed pupils; Grade 1, unilaterally fixed with a fixed pupil diameter >7 mm; Grade 2, unilaterally fixed with a fixed pupil ≤7 mm; Grade 3, unilaterally sluggish; Grade 4, a bilaterally brisk response; or Grade 5, normal response. The length of time between trauma onset and decompression was obtained by reviewing information recorded by the National 119 Rescue Service and operation records. Early decompression was defined as being treated within 3 hours after trauma onset; late decompression was defined as being longer than 3 hours. Survival was defined as living at more than 3 months after DC, and the cause of non-survival was not considered in this study. Statistical analysis was conducted using the paired Student t-test, chi-square test, and the level of statistical significance was set at p<0.05.
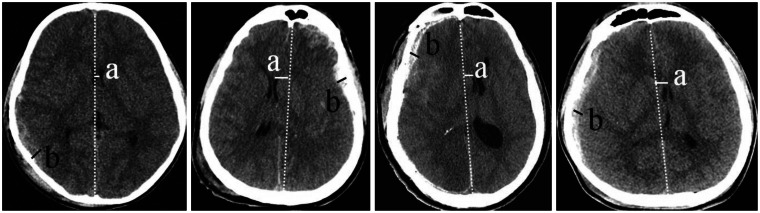 | FIGURE 2Diagram of brain compression ratio with acute subdural hematoma (ASDH). a: the distance between the most medial side of the caudate nucleus head and an imaginary midline from the anterior to posterior falx at the level of the frontal horn of the lateral ventricle, b: the distance between the most lateral side of ASDH and the inner skull table at the same level where parameter a is measured.
|

Go to :
Results
The relationships between the studied variables and survival after DC in 133 cases of ASDH are shown in Table 2. In total, 108 cases were male and 25 were female (M:F=4.32:1); no statistical difference in survival was observed between the sexes (p=0.230). Variations in age were evaluated according to age younger or older than 40 years, as well as to age younger or older than 50 years. When evaluating survival according to age younger or older than 40 years, survival was not different between the two groups (p=0.659). When evaluating survival according to age younger or older than 50 years, however, a significant difference in survival was observed between the two age groups (p=0.012). The positive and negative likelihood ratios for those younger than 50 years old were 1.578 and 1.041. Variations in brain compression ratio were evaluated utilizing the criteria of 0.5 and 1.0. Using the criteria of 0.5, survival was not different between those with a ratio of less than 0.5 or greater than 0.5 (p=0.716). A survival difference was observed, however, between those with a brain compression ratio of less than 1.0 and those with a brain compression ratio greater than 1.0 (p=0.042). The positive and negative likelihood ratios for a brain compression ratio of less than 1.0 were 1.358 and 0.679, respectively. An increased survival difference was also observed for those with a brain compression ratio of less than 1.5, with positive and negative likelihood ratios of 1.243 and 0.204, respectively (p=0.019). The absence of brain stem compression was also shown to contribute to survival with positive and negative likelihood ratios of 0.754 and 0.525, respectively (p=0.020). The time interval between trauma onset and operation and initial GCS were not correlated with survival rate. Although variations in the time interval between trauma onset and the operation was evaluated by the criteria of 2 and 3 hours, no significant survival improvement was observed (p=0.835 and 0.563, respectively): preoperative GCS as 8.0±2.6 and 8.9±2.1 in lesser and more than 2 hours of time interval (p=0.137), and 8.8±2.4 and 8.7±1.9 in lesser and more than 3 hours of time interval between trauma onset and decompression (p=0.834). Variations in initial GCS was evaluated by three criteria, and no survival difference was observed (p=0.366, 0.437, and 0.554). Among the 133 cases reviewed, only patient age (younger than 50 years old), brain compression ratio (less than 1.0), and a non-compressed brain stem were shown to be related with improvements in survival rate after DC in patients with ASDH.
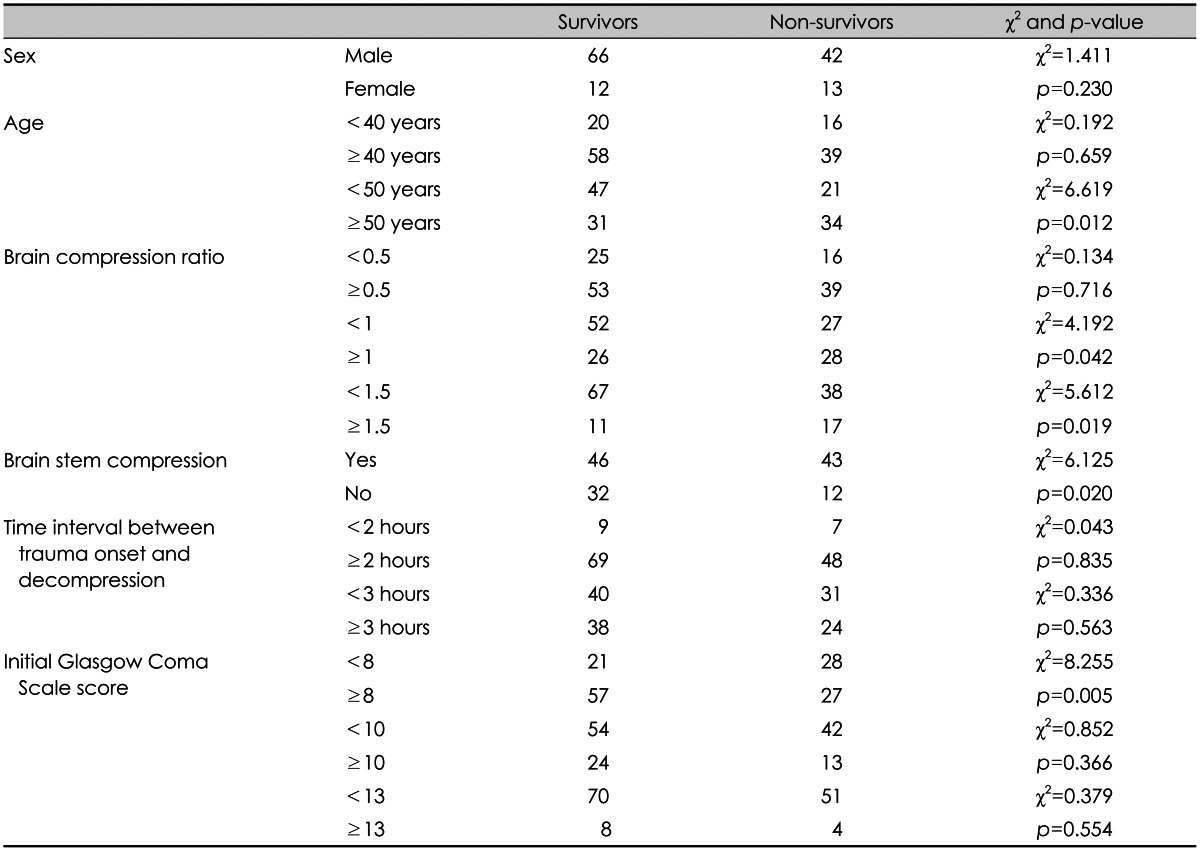
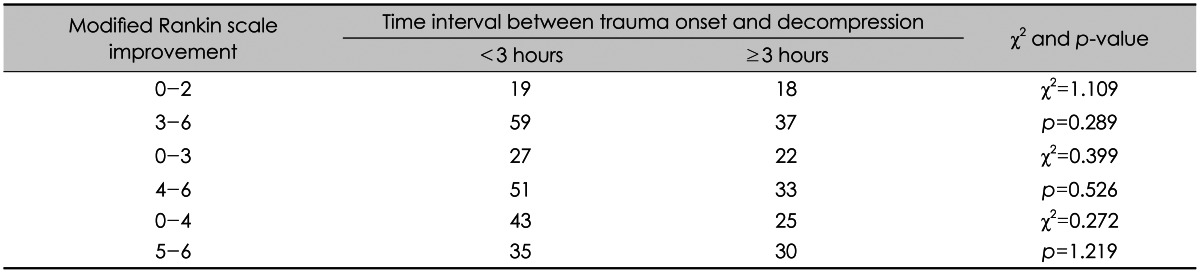
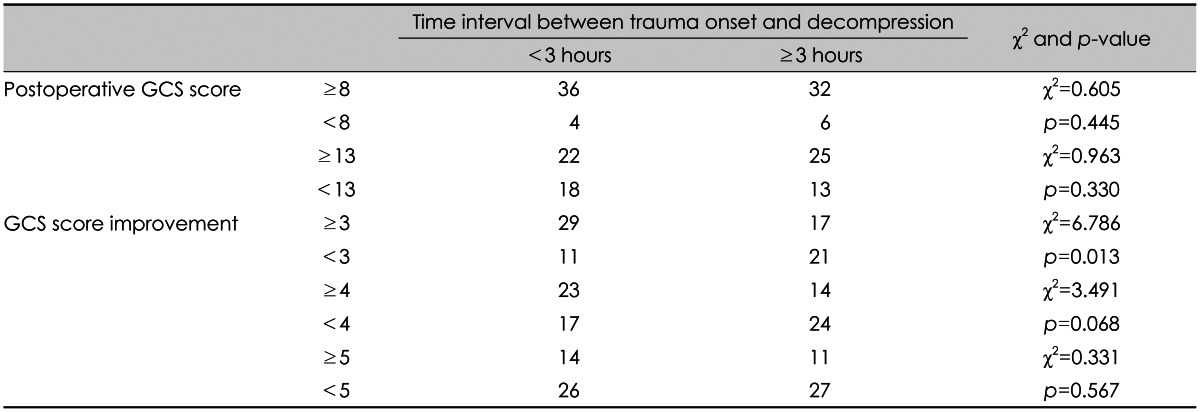
Table 3 shows the relationships between the mRS and the time interval (3 hours) to DC in 133 cases with ASDH. The time interval between trauma onset and operation was not related with the mRS. Table 4 summarizes the relationships between neurological improvement and the time interval between trauma onset and decompression in 78 survivors treated with DC for ASDH. The time interval between trauma onset and operation was not related with a postoperative GCS score of more than 13. However, this interval was closely related to improvement in GCS score. Among the survivors of DC, improvements in GCS score of more than three points compared to preoperative measurement were more frequently observed among the early (less than 3 hours between trauma onset and operation) decompressed cases (29 out of 40 cases of early decompression vs. 17 out of 38 late decompression cases, p=0.013). However, improvements of more than 4 or 5 points on the GCS were not affected by early decompression (p=0.068 and 0.567).
Go to :
Discussion
DC is commonly performed as a management option for TBI.10) Several reviews have been conducted to determine when to perform DC based on radiological findings and the neurological status of the patient.814162131) Indeed, there have been several reports of poor outcomes in patients who underwent DC for TBI,2842) and therefore, it has been difficult to reach a consensus on whether DC should be considered in the management of refractory ICP in TBI.14)
Previously, DC was shown to decrease ICP and improve neurologic outcomes in an animal model of TBI.46) In patients with TBI, improved outcomes after DC have been reported in some case series,13142025) but not in others.3133745) One recent series reported favorable outcomes in 50 patients after DC when other medical measures had failed to control ICP.1) Improved outcomes after DC are also supported by single-center case-control studies.3135) However, DC surgery is not free of surgical complications, and published series suggest a mean incidence of 7% for infection requiring bone removal, 6% for meningitis/encephalitis, and 20% for hydrocephalus requiring a shunt.3121417262931374344) In adults with refractory brain swelling after TBI, it is currently unclear whether DC improves outcomes. Nonetheless, this surgery has been variably performed despite uncertainty on its efficacy, timing, and neurologic outcomes among survivors. Unfortunately, the current study was not designed to compare these relationships between DC and non-DC cases. However, multicenter randomized controlled studies, such as DECRA (DC pilot study) are underway, and meaningful results are expected.9)
The main purpose of the present study was to investigate associations between survival rate and other related factors, as well as to evaluate the effects of early decompression on ASDH. According to previous reports, patients may exhibit better outcomes when they receive DC early after sustaining an injury,31) the rationale being that effective ICP control might improve patient outcomes only if initiated before pressure related secondary brain injury occurred.35) However, the literature has shown this to be untrue. In particular, Cavuşoğlu et al.6) recorded high overall morbidity and mortality rates despite the performance of early decompressive procedures. Additionally, Eberle et al.11) reported that the timing of DC showed no clear trend, for either good neurological outcomes or death, with an overall survival rate of 74.4% and favorable neurological outcomes in 41.9%. Cooper et al.8) concluded that early DC decreased ICP and length of stay in the ICU, but was associated with more unfavorable outcomes in adults with severe diffuse TBI and refractory intracranial hypertension. A prospective study of early versus late craniectomy in TBI by Wen et al.38) also reported that early DC did not improve patient outcomes when compared to late DC for managing TBI. Cianchi et al.7) also reported negative results with comparable 6-months neurological outcomes in late craniectomy patients with refractory intracranial hypertension. Unfortunately, similar results were also observed in the present study, as the time interval between trauma onset and operation was not shown to be related to survival rate in ASDH patients with DC. Moreover, the mRS was also not correlated with this time interval. Instead, survival rate was only shown to be related with patient age (younger than 50 years old, p=0.012), brain compression ratio (less than 1.0, p=0.042) and absence of brain stem compression (p=0.020).
Despite the above, we obtained a new perspective on the effects of early decompression in ASDH. In this study, the time interval between trauma onset and operation was closely related with improvement in neurologic scores on the GCS. Among the survivors, improvements in GCS score of more than three points, compared to preoperative measurement, were more frequently observed among the early (less than 3 hours between trauma onset and operation) decompressed cases (p=0.013). Similarly, Xiao et al.41) in addressing the effect of DC on long-term functional outcomes, discerned that early decompression should be performed in patients before herniation occurs. Additionally, Csókay et al.10) also reported the importance of very early DC in the aspect of ICP increase prevention in children with severe traumatic brain swelling. Accordingly, early DC may offer useful advantages to patients indicated for DC, although we are unable to define exactly what these are at this time. Future studies from this perspective may be able to fill in the gaps in knowledge that prevent us from outlining such benefits.
This study has a few limitations that deserve consideration. First, this study was a single-center consecutive study, and the results obtained from the analysis of the available data are limited by their lack of reproducibility in a randomized, prospective study sample. Secondly, the data was retrospectively reviewed without consideration for combined disease, so the real cause of death was not clear and the real non-survival rate induced by brain injury is unknown. Nevertheless, despite these limitations, this study was able to establish justification for early DC in ASDH patients.
Go to :
 XML Download
XML Download