

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Although chronic subdural hematomas (CSDHs) are a frequently encountered neurological condition, there has yet to be a firm consensus regarding the optimal surgical technique for the treatment of this disorder.1121820) However, based on the disease-prevalent population, surgical morbidities, and recurrence after surgery, less-invasive surgical techniques have become the initial procedures of choice.912171923) Closed-system drainage using burr hole craniostomy (BHC) or twist-drill craniostomy (TDC) have been recommended as first-choice treatments for CSDHs, but the method chosen is based on the surgeon's preference.
We have proposed that a safe entry point for the treatment of CSDHs using TDC is 1 cm anterior to the coronal suture at the superior temporal line.6) This entry point, which is known as the pre-coronal suture entry point (PCSEP), allows for safe trephination due to prominent skull landmarks as well as the preoperative estimation of hematoma thickness using a brain computed tomography (CT) scan. The safety and technical usefulness of TDC at PCSEP have been confirmed in the literature.813) Thus, the aim of the present study was to determine the surgical experiences and patient outcomes of prospectively collected data for consecutive patients who were treated by the surgeon who originally developed the PCSEP approach.
Go to : 
Materials and Methods
The present study enrolled patients with surgically-treated CSDHs who were managed by a single surgeon (senior author: SCH) and whose data were prospectively collected over 5 consecutive years. The symptomatic CSDHs of 86 patients who had follow-up periods of more than 3 months were included in this study. When the hematoma had a thickness of more than twice that of the skull at the normal entry point, the first-choice technique was TDC via the PCSEP, which was 1 cm anterior to the coronal suture in the superior temporal line. This point is easily indicated on a brain CT scan and on the patient's scalp. If TDC was not possible, BHC was performed at the parietal entry point because this area would be more aesthetically acceptable for a longer scalp incision and the postoperative depression of the skull. Additionally, on trying TDC at the parietal area, we did not intend to make an injury to the meningeal vessels and penetrate the brain when the exact thickness of the hematoma was uncertain. The choice of procedural methods for treating the CSDHs was simplified by using TDC at PCSEP as the primary treatment option and BHC at the parietal bossing area as a secondary treatment option. The clinical characteristics of both groups were assessed to determine how many TDC procedures were performed in consecutive CSDH patients and the reasons that BHC would be performed as secondary option.
Surgical procedures
The TDC surgical procedure used in the present study was identical to that previously described by our research group.6) The PCSEP was marked on the scalp, hematoma thickness at the PCSEP was easily determined using a brain CT scan, and TDC was performed if the thickness of the hematoma was more than twice the thickness of the bone. After scalp preparation with alcohol and a povidone-iodine solution, a solution of 2% lidocaine was applied, and a stab incision approximately 5 mm in length was made with a No. 15 scalpel at the entry point. First, the skull and dura were penetrated in a perpendicular manner with a hand drill to avoid the twist-drill's slipping down the skull and separating the dura from the skull. Then, the twist-drill trephination was made at a 45° angle to the surface of the bone to prevent the indwelling catheter from entering the cortex; the usual direction is posteroinferior toward the auricle. A standard ventriculostomy catheter (No. 5) was introduced into the subdural cavity at a depth of approximately 5 cm, and the contents were allowed to flow freely to and fro according to the up and down movement of the catheter. Neither aspiration with negative pressure nor flushing with normal saline was performed.
For the BHC procedure, a vertical scalp incision was made on the parietal bossing area, and a burr hole was created with an air drill. Following the dural incision, the ventriculostomy catheter was inserted into the hematoma cavity in an anteroinferior direction. No irrigation was done through the burr hole.
Go to :
Results
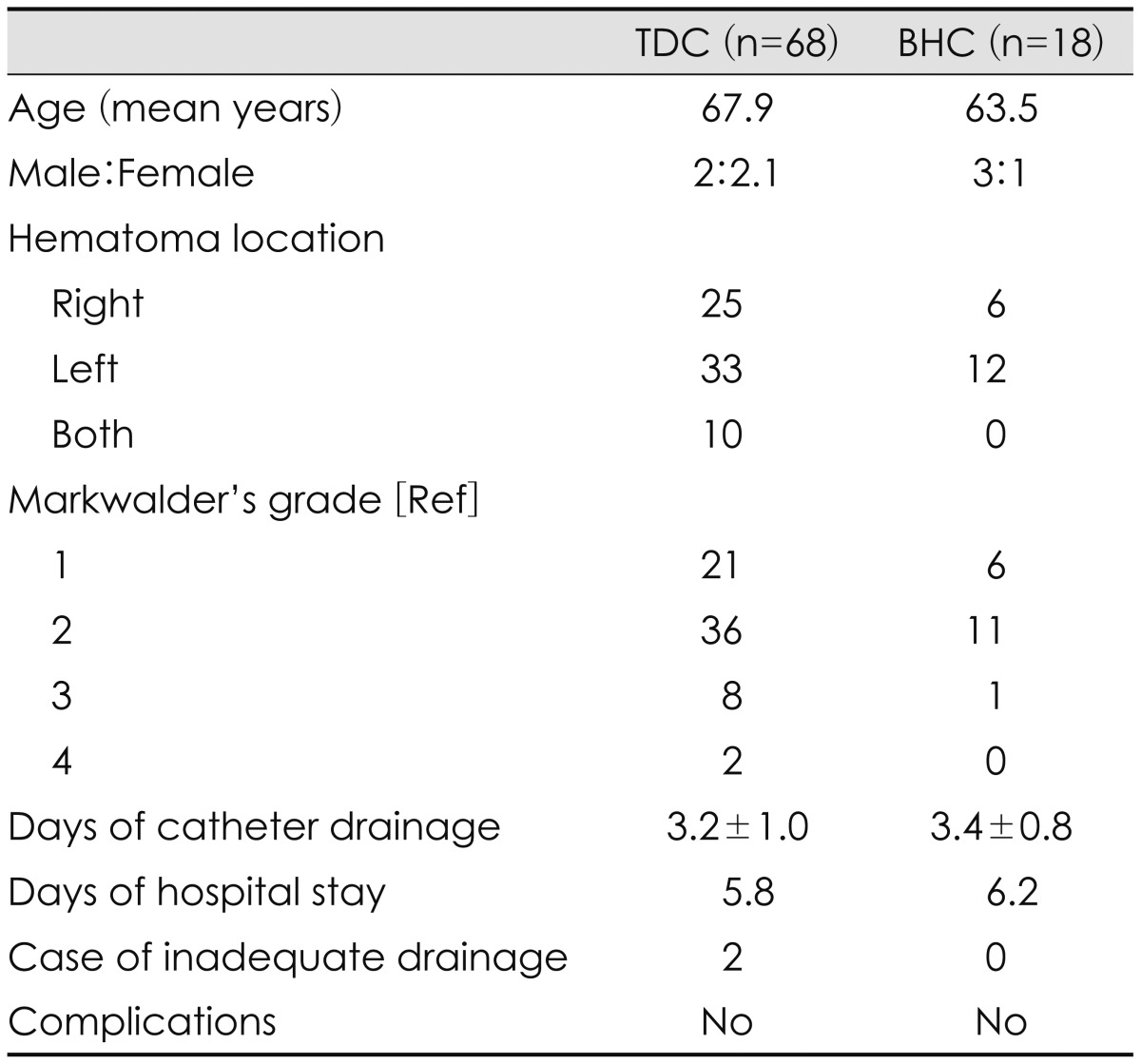
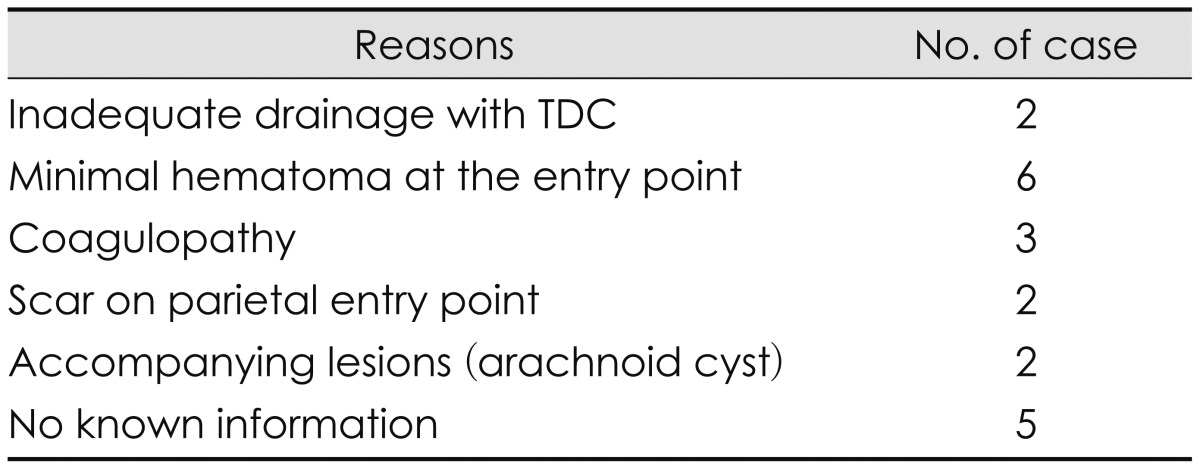
The present study included 86 patients; 68 (79.1%) were treated by TDC, and 18 (20.9%) by BHC as the initial treatment method (Table 1). All patients showed improvements in their symptoms after hematoma drainage. Furthermore, no morbidity or mortality was associated with either technique, and there were no differences in duration of drainage days or hospital stay between the groups (Table 1). Remarkably, no BHC procedures were necessary for patients with bilateral CSDHs because each of these cases had enough thickness at the PCSEP to accommodate the trephination and insertion of a drainage catheter. The reasons for the performance of BHC in 20 patients are shown in Table 2; in two cases, the hematomas were insufficiently drained by the initial TDC procedure and, subsequently, BHC was performed at the parietal entry point 1 day later. Six patients had hematomas (7% of 86 hematomas) that did not exhibit sufficient thickness on the CT scan to warrant a TDC procedure. Three had the coagulopathy as an underlying disease, so burr hole drainage was done as the first treatment. Two had a previous scar on the parietal entry point, two had associated lesions (such as an arachnoid cyst), and a retrospective analysis could not identify the reason for a BHC as the first-choice option in five patients. So, twelve hematomas of those patients could be drained by TDC instead of BHC as a first treatment method.
Go to :
Discussion
The drainage of CSDHs can be accomplished by two craniostomy methods: the burr hole and twist-drill techniques. Because there are no significant differences in the effectiveness of these two techniques,112) the surgeon's preference determines their use. Thus, the present study aimed to determine the safety and feasibility of TDC at the PCSEP as a first-choice treatment option for CSDHs using 86 prospectively enrolled patients. TDC was attempted in 79.1% of the patients in the present study. However, approximately 93.0% (80 of 86) of the patients may have been treated with the TDC technique if the BHC cases had been treated with TDC, except for six patients with minimal hematomas at the PCSEP. Only 7% of the hematomas exhibit not enough thickness at the PCSEP on a brain CT scan to consider the use of TDC. In our case series for draining CSDHs, only 2 cases had insufficient drainage by initial TDC procedure. Nonetheless, the BHC cases decreased as the opportunities to perform TDC increased.
Because a craniostomy is a relatively less invasive procedure, it is the favored treatment method for symptomatic CSDHs. Surgery and anesthesia entail the invasive techniques and are associated with medical complications; thus, the least invasive operative therapies for CSDHs hypothetically offer the best chance to reduce mortality after surgery.182124) The use of a postoperative continuous closed-system drainage following TDC or BHC offers substantial advantages for the treatment of CSDHs by allowing the brain to sufficiently re-expand and fill the subdural space.22) Additionally, the closed catheter drainage system reduces the likelihood of a recurrence of the hematoma.1912) The incomplete removal or reaccumulation of a hematoma frequently occurs after BHC,1821) but the maturation of the neomembrane can be a primary mechanism underlying the spontaneous resolution of a remnant hematoma that can prevent hematoma reaccumulation.9) Operations that are relatively more invasive, such as larger craniotomies, are not more effective in terms of hematoma evacuation, the avoidance of hematoma reaccumulation, or neurological improvement.4) In fact, rebleeding from the hematoma neomembrane makes the incomplete removal and/or reaccumulation of a hematoma effectively inevitable regardless of the surgical method.18) Taken together, these findings suggest that the simple continuous drainage of CSDHs is the treatment of choice, even though there are no significant differences in the recurrence rates after BHC and TDC.1)
TDC is an effective treatment modality for CSDHs,192122) and if the TDC procedure ensures the safety of the patient during the operation, then it can be a first-choice treatment option for CSDHs. Before the PCSEP was introduced as a normal entry point, craniostomy procedures were performed in indefinite areas, such as the rostral or anterior aspects,2523) or the site of maximal thickness of the subdural hematoma.161925) The indefinite nature of these procedures resulted in what would be an essentially blind TDC operation in which the site of trephination may be in a different location than that determined by the preoperative design and may be in an area along the dural vasculature. As a result, surgeons neglected the advantages of the TDC operation, such as a shorter procedure time, less scarring, and the avoidance of air entrapment.16) Air entrapment is a risk factor for recurrence.15)
The PCSEP, which is 1 cm anterior to the coronal suture at the level of superior temporal line, has many advantages including anatomical safety and a navigating landmark. First, because it is located at a relatively frontal position, the procedure can be performed in the supine position, and the patient feels comfortable and can be easily monitored if sedated. Second, both sides of the PCSEP can be trephined without a surgical position change in the case of bilateral hematoma; in the present study, all of the bilateral hematomas were treated by TDC. Third, the PCSEP is close to the coronal suture, which enhances the adhesion of the dura to the skull and results in decreased risks of dural detachment and postoperative epidural hematoma. Finally, the shorter procedure time for TDC, with a mean operation duration of only 8.9 minutes,13) may obviate the need for monitored or general anesthesia, especially in confused or elderly patients. Additionally, even though a patient may be bald in the frontal region, TDC may not be contraindicated because it involves a stab incision and not a bony depression.
Although CSDHs are generally considered benign,31114) many elderly patients suffer from this disorder and exhibit a high mortality rate for up to 1 year after their diagnosis relative to the anticipated actuarial survival.14) This suggests that CSDHs are a marker of other underlying chronic diseases, such as hip fracture. However, we found that many patients included in the study do not undergo surgery (34.4%), some have a relatively high in-hospital mortality rate (16.7%), and few return home (21.1%).14) Nonetheless, the surgical drainage of CSDHs in nonagenarians and centenarians is associated with a lower incidence of inpatient death and higher 30-day and 6-month survival rates.10) And none of the patients in the conservative care group showed any neurological improvement10); thus, the aggressive surgical drainage of symptomatic CSDHs may enhance the survival of elderly patients.
In the elderly, coexisting systemic diseases typically pose a problem under general anesthesia. Although there are no significant differences in terms of surgical complications between patients who receive local and general anesthesia, those who undergo general anesthesia exhibit more cardiovascular complications and longer hospitalization periods.7) Thus, the shorter procedural duration of TDC and the absence of sedation or general anesthesia during the procedure may help reduce the morbidity. The draining of a hematoma should be not accompanied by morbidity that could result in a high mortality rate, and the least invasive and shortest procedures should be considered as first-choice treatment options, while more invasive surgical techniques should be reserved for more complicated situations. Thus, it is proposed here that TDC at the PCSEP should be considered a first-choice treatment option for patients with CSDH, especially if they are elderly.
Go to :
Conclusion
In conclusion, the majority of the CSDHs in the present study were effectively treated by TDC at the PCSEP and a closed drainage system when the hematoma was of sufficient thickness. Thus, the present findings suggest that TDC at the PCSEP should be considered a first-choice treatment option for CSDHs, especially in elderly patients, while BHC at the parietal entry point should be reserved for more complicated cases.
Go to :
 XML Download
XML Download