

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
With the increasing popularity of sports worldwide, greater attention has been paid to sport-related head injuries. The number of adults participating in sports has gradually been increasing in Japan. According to a recent survey in Japan, the number of adults participating in sports at least once a week is 47.5%. In Japan, sports are promoted by maintaining a sporting environment in the community, encouraging play against international competitors, and supporting the link between physical education in school and lifelong participation in competitive sports. In this context, the number of elementary and junior high school students experiencing head injuries has increased. Ensuring appropriate sport-related head injury management becomes more important as the number of participants grows, and neurosurgeons need to have a sufficient understanding of these injuries.
In this article, we reviewed it about the acute subdural hematoma (ASDH), traumatic cerebrovascular disease, concussion, chronic traumatic encephalopathy (CTE) in sport-related head injuries.
Go to : 
Acute Subdural Hematoma
The majority of ASDHs due to sport-related head injuries are simple ASDHs without cerebral contusion and typically occur during contact sports. The patient sustains a major blow to the occipital region of the head when thrown to the ground. The resulting rotational acceleration of the brain in the anteroposterior direction can cause separation of the brain and dura mater, with consequent rupture of the bridging veins (Figure 1). A survey of judo accidents revealed that 28% of the injured players had experienced headache before the accident, suggesting that some of them were susceptible to bridging vein rupture due to preexisting mild head cerebral injuries from earlier head traumas (Figure 2).
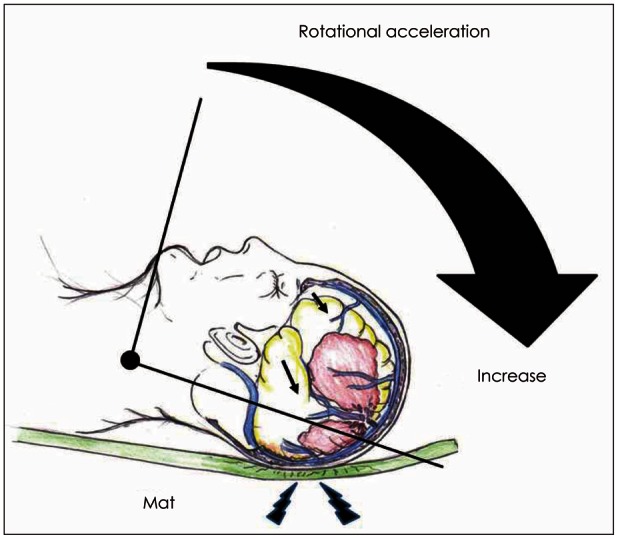 | FIGURE 1Rotational acceleration injury and damage to the bridging vein with the neck as a pivot point during judo. When the head strikes the mat, rotational acceleration is increased in brain (arrows), putting tensile strain between the bridging vein and dura mater, leading to rupture.
|
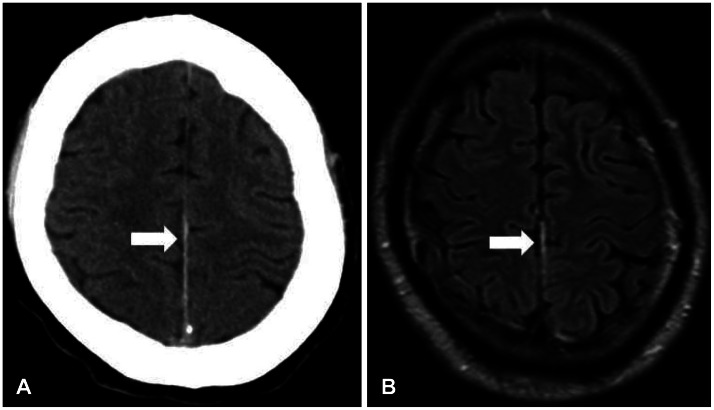 | FIGURE 2A 30-year-old man was admitted to the hospital with mild headache and amnesia. He had been thrown by a judo competitor and received a blow to the back of the head 4 hours before presentation. Computed tomography (A) and fluid-attenuated inversion recovery magnetic resonance imaging scans (B) on admission revealed a thin subdural hematoma in the interhemispheric fissure (arrows).
|
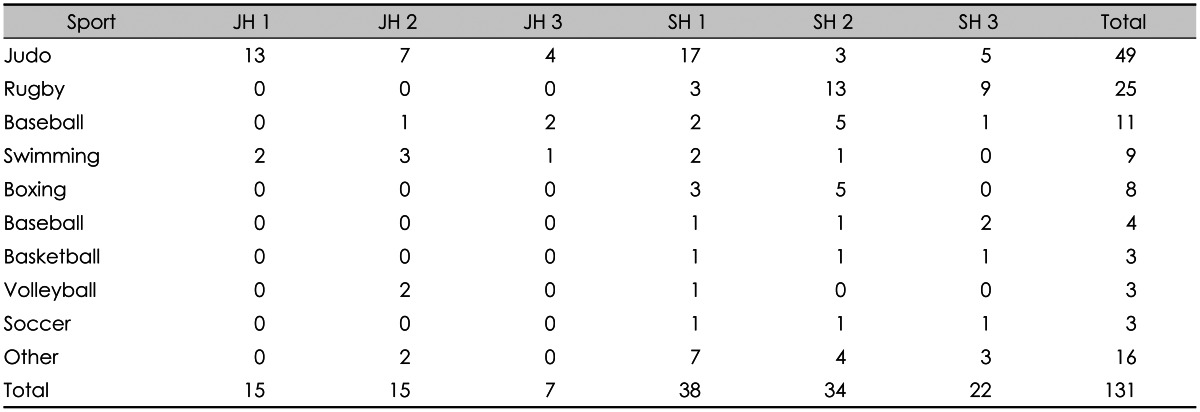
Severe head injuries are prevalent in contact sports such as American football, rugby, boxing, judo, ice hockey, skiing, and snowboarding. In the United States, severe head injuries in sports are most commonly associated with American football, and a reported 90% of cases are ASDHs. Furthermore, the number of cases is increasing annually. In the United States, almost all patients with ASDH due to sport-related head injuries are senior high school students or younger.16) ASDH in Japanese sports is most commonly associated with judo, with novices and younger players at high risk (Table 1), especially when they practice with other stronger and more advanced students.17)
Go to :
Traumatic Cerebrovascular Disease
Cerebral infarction during sport participation is very rare. Most cases reported to date have been in male athletes, and approximately 80% of the patients were diagnosed with ischemia or infarction due to arterial dissection.1) This condition has been observed in a wide variety of sports including yoga, tennis, soccer, rugby, kendo, judo, karate, winter sports, bowling, wrestling, scuba diving, and taekwondo.4) The most frequent causes of common and internal carotid artery dissection were blunt trauma and rotational impact, and symptoms included amaurosis, transient ischemic attack, middle cerebral artery infarction, headache, facial pain, anterior neck pain, and Horner's syndrome.9) One report describes vertebral artery dissection due to rotational impact while playing golf. Computed tomography (CT) angiography, magnetic resonance angiography, and ultrasound are useful for diagnosing arterial dissection. Ultrasound is particularly useful for detecting common and internal carotid arteries dissection.21) We recommend that athletes with a history of arterial dissection not participate in active sports, especially those that require neck rotation or hyperextension.11)
Go to :
Concussion
It is estimated that 1.6 to 3.8 million sport-related concussions occur annually in the United States,8) accounting for 5 to 9% of all sport-related injuries. Concussion was previously regarded as a mild head injury that causes temporary loss of consciousness and amnesia and spontaneously resolves with time, and the risks associated with this injury were historically underestimated. However, recent years have seen a major change in the global attitude toward concussion.12) Studies have shown that athletes who had suffered multiple concussions in contact sports such as American football, boxing, ice hockey, basketball, and soccer exhibited neuropsychological abnormalities, and some went on to develop CTE.14) These findings have resulted in greater attention paid to concussion for both social and medical reasons.5781012)
Considering that some patients with sport-related concussions may develop fatal brain edema,15) proper management of this condition is critical. A clear understanding and thorough evaluation of the condition is mandatory for athletes, coaches, and trainers. Recently, sport organizations such as the Fédération Internationale de Football Association, the International Ice Hockey Federation, the International Olympic Committee, and the International Rugby Board have developed guidelines for concussion management that include strict and detailed criteria for returning to sports. In our view, sports medicine doctors and neurosurgeons who evaluate patients with concussions and other sport-related head injuries should have a sufficient understanding of concussion assessment and the criteria for returning to sports. Currently, concussion is regarded as a head injury defined as a complex pathophysiological process affecting the brain that is induced by traumatic biomechanical forces. A concussion is caused by a direct blow that generates an impulsive force that is transmitted to the head. The most frequent symptom is headache, followed by dizziness. The incidence of loss of consciousness is as low as 10%.12) Although 80% of patients become asymptomatic within 10 days without treatment,19) 10 to 20% experience persistent symptoms for several weeks or even months.18) Once a concussion occurs, the risk of a second event is 2 to 5.8 times higher compared to individuals with no concussion history.6) Patients with more frequent concussions are likely to have more severe and prolonged symptoms. Repeated concussion is considered to increase the risks of both functional decline and structural/microscopic anatomical brain damage, and the accumulated brain damage can cause CTE with apparent brain atrophy that may lead to cognitive and psychiatric disorders and motor symptoms such as Parkinsonism.14)
Concussion diagnosis
According to the consensus statement of a recent international conference, concussion is suspected when an individual has at least one of the following signs and symptoms:12)
When a concussion is suspected during a sporting event, a coach, trainer, or other professional should immediately perform an assessment using tools such as the Pocket Concussion Recognition Tool. When physicians or other healthcare professionals assess patients with suspected concussion, they should use more specialized tools such as the Sport Concussion Assessment Tools (SCAT; currently updated as SCAT3 and child SCAT3) developed by the International Conference on Sport Concussion. When a concussion is suspected, the athlete should not be allowed to return to sporting activities that day. In addition, continuous monitoring is necessary for at least several hours to reduce the risk of exacerbation. In the medical setting, head CT or magnetic resonance imaging (MRI) should be performed to rule out organic lesions. Diagnostic imaging is highly recommended to exclude the possibility of brain injuries such as ASDH and cerebral hemorrhage, especially when the individual has a persistent headache.12) Coronal CT and MRI scans are useful for identifying hematomas near the tentorium or bridging veins in the middle parietal region.
Return to sports after a concussion
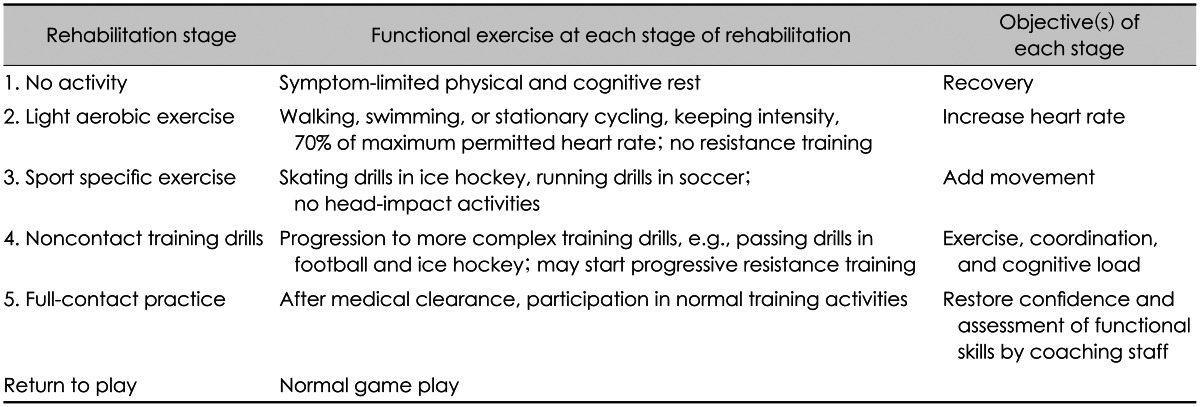
Athletes are not allowed to return to sports unless their symptoms have completely remitted. After full symptom resolution, they should return to sporting activities in a stepwise manner according to graduated return to play protocol (Table 2).12) Each step of the protocol requires 24 hours, and the process stops if there are any symptoms. Therefore, at least 1 week is required to return to sporting activities. In the final stage, the athlete undergoes a medical check-up before they are cleared to return to their sport. If any symptoms are observed, the athlete is ordered to rest and return to the previous stage of the protocol.
Go to :
Chronic Traumatic Encephalopathy
CTE is a progressive degenerative disease typically found in subjects with a history of repeated head injuries including concussion during contact sports.13) In 1928, Martland first reported this condition in boxers who developed motor and cognitive impairment following repeated blows to the head; it was also referred to as punch drunk syndrome. The term CTE has been used since the 1960s to describe the condition in all athletes participating in sports with a high risk of concussion, such as American football, professional wrestling, and professional ice hockey. Symptoms of CTE usually develop over several years (i.e., 10 or more) after repeated head injuries. The initial symptoms consist of mental disorders including depression, apathy, irritability, suicide attempts and ideation; behavioral disorders including impulse control disorders (being easily angered and/or unable to control emotions), disinhibition, and violence; and cognitive disorders including learning disabilities, memory disturbance, and other higher brain function disturbances. Patients begin to show progressive symptoms in their 30s to 50s.2) Over time, motor symptoms such as balance disability, extrapyramidal disorder, dysarthria, and other speech abnormalities start to appear. Patients in the advanced stage exhibit brain atrophy in the frontal and parietal lobes, basal ganglia, and mammillary bodies. A septum pellucidum cavity with spinal fluid retention is observed in many patients. Pathological examination shows accumulation of tau protein and TAR DNA-binding protein-43 in the frontal and temporal lobes, brain stem, basal ganglia, cerebellar dentate nucleus, as well as neuritis.20) Repeated brain concussions are not the sole cause of CTE development and progression; other factors are thought to be involved in its pathogenesis, although these remain to be clarified.
Go to :
Return to Sports after Organic Brain Damage
In theory, athletes who have suffered organic brain damage or an ASDH should not be allowed to return to contact sports with a high risk of concussion (e.g., boxing, karate, judo, sumo, rugby, American football, soccer, ice hockey, snowboarding), even after full resolution of the symptoms and in the absence of lesions on imaging studies (Figure 3).3)
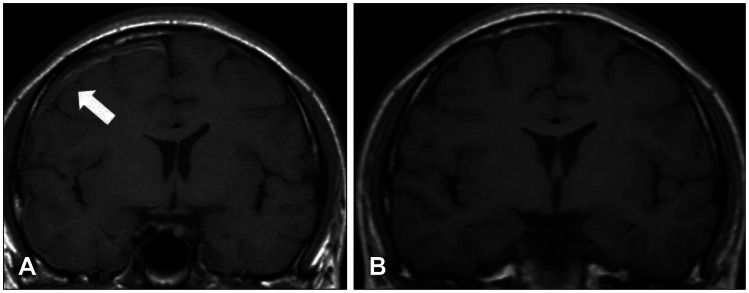 | FIGURE 3A college-level judo athlete presented with a persistent headache after practice. Fluid-attenuated inversion recovery (FLAIR) magnetic resonance imaging (MRI) revealed a thin subdural hematoma on the right convexity (A, arrow). He was treated conservatively. Four months later, his symptoms remitted, and FLAIR MRI showed no evidence of a subdural hematoma (B). He returned to judo practice 6 months after his initial injury but suffered fatal acute subdural hematoma during judo practice.
|
Go to :
Conclusion
Since severe head injuries sustained while participating in sports frequently affect novices and younger athletes, education on head injury management is important for both instructors and athletes. For example, judo students should be taught self-defense techniques such as ukemi (applied while being thrown). The most important point is to not underestimate the risks associated with concussion. When a concussion is suspected, the athlete should not be allowed to return to sporting activities on the same day, and a structured protocol should be followed before they can participate again. In particular, it is crucial to prevent head injury exacerbation due to early return to sporting events. The data presented in this review underscore the need for neurosurgery to prevent and manage sport-related head injuries.
Go to :
 XML Download
XML Download