

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Craniocerebral gunshot injuries (CGI), initially described and managed in military settings, are now increasingly encountered by neurosurgeons in civilian and urban settings, been on the rise especially in developing countries. Although less prevalent than closed head trauma, penetrating brain injury carries a worse prognosis.52) CGI are the most lethal of all firearm injuries, with reported survival rates of only 7% to 15%.61)
About 90% of the time, the victims die before arriving at the hospital, and for those who survive and make it to the hospital, about 50% die in the emergency room.1162) Peak mortality from CGI happens at the scene or within 3 hours of injury.1140) This reality requires that management of gunshot (missile) wounds (injuries) of head (craniocerebrum) due to bullets, shotguns, blasts, explosion of grenades and mines must be a routine experience in any Neurosurgical centre in countries with civil armed conflict. Since patient epidemiology is a multifactorial phenomenon and influenced by psychological, socioeconomic, as well as cultural factors, the characteristics of CGI patients might be fundamentally different between all the continents.
There are many lessons to be learnt. This review considers current ballistic aspects and aspects based on the pathophysiology and related to the diagnosis and management.
Go to : 
Ballistics and Pathophysiology
Projectiles are pellets fired from a shotgun, bullets from rifles, machine-guns, carbines, automatic guns and shrapnel and splinters by exploding bombs, mines and grenades. A missile is a projectile of either a high velocity (muzzle velocity >600 m/sec) or a low velocity (muzzle velocity <300 m/sec).6)
Ballistics
As most of the penetrating brain injuries are caused by missiles or projectiles, an understanding of ballistics (i.e., the study of the dynamics of projectiles) is imperative.52)
Firearms can be classified in many ways; the simplest is according to their speed:
1) Low velocity: less than 1,000 feet per second (<300 m/sec) as handguns or hand sizes 22, 38-caliber and 9 mm.
2) Medium velocity: speeds of 1,000 to 2,000 feet per second (300 to 600 m/sec) as the submachine guns.
3) High velocity: more than 2,000 feet per second (600 to 1,000 m/sec) as the AK-47, G-3 or Galil. These have properties such as rotation, oscillation and fragmentation that make them much more lethal.
Physiopathology
The ability of any penetrating object to penetrate the brain, thus is, the primary injury to the brain is dependent on the ballistic properties (kinetic energy, mass, velocity, shape, angle of approach, the characteristics of intervening tissues, etc.) of the projectile and any secondary projectiles, such as bone or metallic fragments.1752)
It is important to consider the energy delivered and the location in the brain to which that energy is imparted. The kinetic energy (wounding energy) is defined by the relationship: E=1/2 mv2, velocity can be represented as E=1/2 m (Vi2-Vr2) where m is the mass of the projectile, Vi is the impact velocity and Vr is the residual velocity in the case of perforating wound.2742) This implies that the velocity of the projectile has a greater influence than the mass of the projectile alone, meaning that the bullet of an AK-47 assault rifle, which weighs 7.9 g and has an initial velocity of 720 m/s, has a kinetic energy of 2,635 ft/lb (3,573 J). Projectile velocity from firearms in handguns is less than that of rifles, varying usually from 180 m/s to 450 m/s.
When the velocity exceeds 700 m/s, the wounding energy of the projectile is significantly increased, causing more severe brain damage, more bone fragmentation, and enhanced secondary brain cavitation.112) Higher velocity projectiles will also impart an additional temporary cavitation effect in their trail,17) which is a velocity-related phenomenon, a high-pressure sonic wave, lasting for microseconds (2 µsec; insignificant), radiates outwards from the point of primary missile impact.69) Expanding (dumdum) and devastator bullets transmit most kinetic energy preferentially at the impact site.64) The missile deposits its kinetic energy on the skull, fragmenting and fracturing the bone, generating small bone pieces (secondary missiles) into brain tissue furthering damage. Adjacent and distant to track, is a low pressure, long (milliseconds) lasting wave which displaces and crushes the brain tissue radially due to moving missile in the brain, thus rapidly compressing it tangentially from the primary track, leading to temporary cavitation and suction of air, skin, hairs and debris into brain parenchyma. Such a phenomenon leads to a large exit wound with a perforating injury.18)
Posteriorly, this temporary cavity collapses upon itself only to re-expand in progressively smaller undulating wave-like patterns. Every cycle of temporary expansion and collapse creates significant surrounding tissue injury to the brain. This can result in shear-like injury of the neurons or can result in epidural hematomas, subdural hematomas, or parenchymal contusions.50) However, a bullet does not need to penetrate the skull to cause intracranial damage; the mechanism of injury in these cases is either blunt force or sending bone fragments into the brain.58) The velocity of the missile is important in tangential wounds, having the ability to release sufficient energy to cause intracranial damage without skull bone damage.24)
A projectile loses its kinetic energy rapidly as it travels through the air because of its resistance.50) This loss of kinetic energy is related to the decrement in its velocity which in turn is dependent on the shape of the projectile. Bullets can be blunt-nosed, half or fully jacketed and hollow tipped to increase mushrooming (deformity), to ensure more damage to the tissue of target. The sharper the nose of a bullet, the less the velocity will be decreased by air resistance. The rounder the nose of a bullet or more irregular the shape (as in shrapnel), the quicker the velocity slows and kinetic energy decreases.
Go to :
Classification
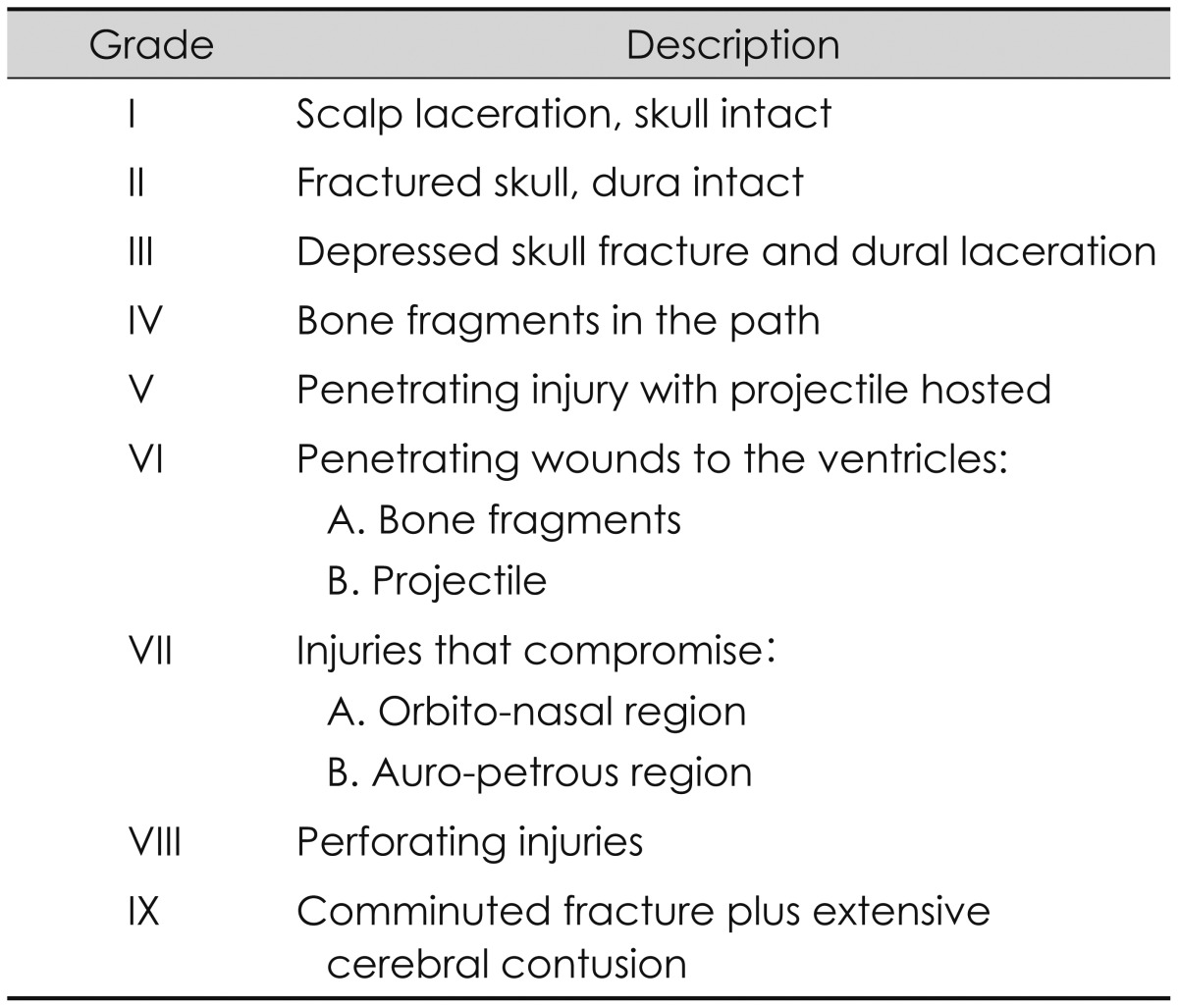
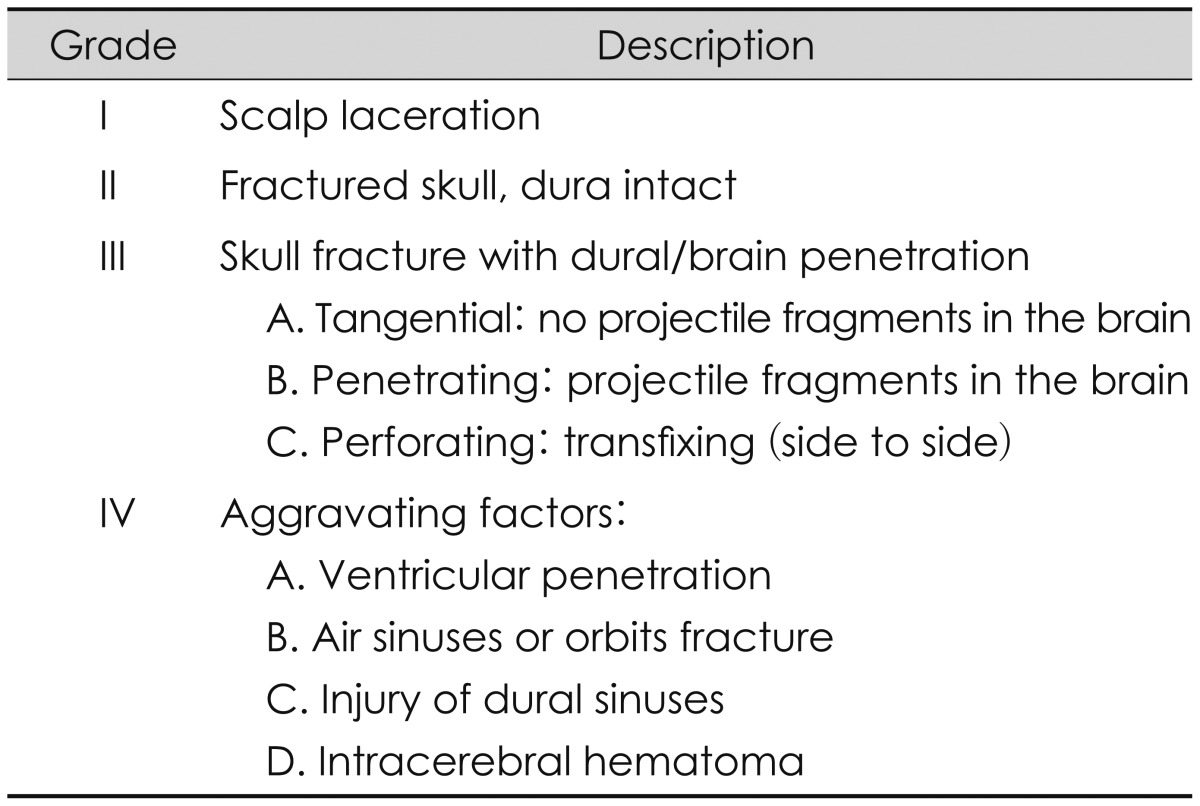
Craniocerebral missile wounds have been classified by Cushing (Table 1), based in his experience on World War I14) and refined by Matson (Table 2) in World War II,38) which is the most currently used. Missile wounds are tangential, penetrating and perforating.538) Penetrating injury is described as gunshot penetrating skull and dura without any exit wound, whereas perforating (transfixing) injury enters the skull and dura and then exits creating both entry and exit wounds. Tangential wounds occurs when a missile grazes the skull at an oblique angle, only lacerating the scalp or stays under scalp causing depressed or elevated fractures and indriving bone fragments into brain parenchyma causing dural tears, cortical contusions, extradural or subdural hematomas.
The preponderance of low muzzle velocity weapons seen in clinical practice and the availability of computed tomographic (CT) evaluation within minutes after presentation has altered the range of prognostic indicators available to the neurosurgeon and the amount of relative importance placed on each factor.62) Raimondi and Samuelson54) in 1970 noted this difference in wound ballistics and offered a classification scheme based on initial neurologic assessment.
Go to :
Neuroimaging
The diverse modalities of neuroimaging used in patients with CGI lies on treatment decision making and for prognostic implications. Neuroimaging is vital for surgical purposes, especially for determine type surgery, size and location of the approach, route of extraction of the foreign body; however not always surgical management is indicated, there is also the not uncommon decision to choose non-surgical management, as will be discussed later. Basic findings that needs determination in CGI include: exit and entry sites; intracranial fragments; missile track and its relationship to both vessels and air-containing skull base structures; intracranial air; transventricular injury; missile track crossing the midline; multilobar injury; basal cistern effacement; brain parenchymal herniation (i.e., fungus cerebri) and associated mass effect.49)
In case of survival, CT scan and magnetic resonance imaging (MRI) can be used to monitor progress and any possible complications, in particular vascular or infectious complications which are specific to this type of injury.20)
Plain films
The availability of CT-scan precludes the use of plain radiography, thus it is not routinely recommended.3559) However, post-mortem radiography is routine and invaluable, particularly when death has occurred prior to the instigation of any emergent medical management and imaging. It has proved invaluable in forensic investigation of gunshot wounds used to locate the bullet, identify the type of ammunition, document the path of the bullet, and assist in retrieval.49)
Brain CT-scan
Brain CT-scan is widely recommended to evaluate patients with penetrating head trauma, in addition to the standard axial view with window bone and brain parenchyma, coronal cuts may be helpful to evaluate lesions of the base and convexity of skull. The literature shows many advantages from CT-scan with respect to skull radiography, including increased capacity to identify missile and bone fragments, characterization of the projectile trajectory, evaluation of the extent of brain injury, and detection of intracranial hematomas (Figure 1). All patients with CGI should be imaged emergently by unenhanced CT whether or not there is evidence of penetration on clinical examination.49) Volume acquisition, is the protocol of choice on current multi-detector helical systems as scanning time is rapid and the volume dataset obtained allows retro-formatting of images to variable section thickness (e.g., for skull-base assessment) as well as three-dimensional surface-rendered fracture depiction.49) CT findings of multilobar injury and intraventricular hemorrhage correlate with poor outcome, as will be discussed in the mortality and prognosis section.2837)
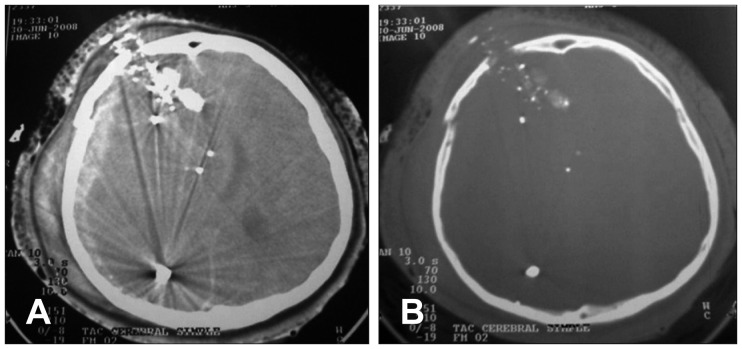 | FIGURE 1Simple brain computed tomography (CT) scan in a case of craniocerebral gunshot injuries. A: Multiple shrapnel from the left region to the right parieto-occipital region, accompanied by subdural hematoma, cerebral edema and ventricular collapse. B: CT bone window, right frontal fracture, accompanied by multiple intracranial shrapnel.
|
MRI
In the acute setting of CGI, MRI is generally not recommended, because it is time consuming and carries the potential danger when there are retained ferromagnetic objects because of possible movement of the object in response to the magnetic torque,17) this consideration is even more important because the majority of military and paramilitary ammunition contains ferromagnetic materials, usually in the jacket covering the lead or antimony core. It has been suggested that bullets showing less deformation on CT or plain film imaging more likely have a hard steel ferromagnetic component compared with the more easily deforming non-ferromagnetic bullets.29) Nevertheless, owing to the uncertainty of bullet construct in the vast majority of civilian shootings, the use of MRI would seem imprudent, and CT should continue to be the primary imaging mode.49)
Cerebral angiography
Angiography (either CT or catheter) may be required in those patients where there is increased risk of vascular injury, this include those cases where the wound trajectory is through or near the Sylvian fissure and, therefore, M1 and M2 segments of the middle cerebral artery, peripheral branches of the anterior cerebral artery, the supraclinoid carotid artery, the vertebrobasilar vessels, the cavernous sinus region or the major dural venous sinuses.4865)
Angiography has a significant role to play in delayed vascular complications occurring following CGI, most notably traumatic aneurysm formation. CT angiography (CTA) has many advantages over conventional catheter angiography. CTA is a rapid, non-invasive, and relatively inexpensive modality; also reveals the trajectory of the wound track and non-vascular injuries. However, there are some limitations of CTA. Streak artifact from shoulders, retained metallic fragments, and dental fillings can prevent adequate visualization of vessels. Also, suboptimal timing of contrast or failed intravenous injection may lead to decreased opacification of vessels, which can impair the detection of vascular injury.60)
Go to :
Treatment
General considerations
Management goals should focus on early aggressive, vigorous resuscitation and correction of coagulopathy; those with stable vital signs undergo brain CT scan.33)
If aggressive therapy results in a high chance of severe disability or persistent vegetative state in survivors with only a very small chance of a good outcome most neurosurgeons would be discouraged from aggressively treating the Glasgow Coma Scale (GCS) 3-5 group.59) Grahm et al.22) recommend in these patients (GCS of 3-5) that after resuscitation should not be treated unless there was an operable hematoma, the economic and psychosocial burden of caring for these disabled survivors is immense.59) Patients with a GCS of ≥8 should be treated aggressively.22) To consider, organ donation after fatal CGI is a legitimate goal.
The treatment can be summarized in 4 steps:
1) Immediate life salvage, through control of persistent bleeding and cerebral decompression.
2) Prevention of infection, through extensive debridement of all contaminated, macerated or ischemic tissues.
3) Preservation of nervous tissue, through preventing meningocerebral scars.
4) Restoration of anatomic structures through the hermetic seal of the dura and scalp.
Intracranial hypertension
Intracranial hypertension (ICH) is the leading cause of death in patients with traumatic brain injury (TBI) and contributes to secondary brain injury if not properly handled. The Monroe-Kelly doctrine suggests that the rigid skull is occupied by three volumes: blood, brain and cerebrospinal fluid (CSF), at least any additional volume, such as hematomas, cerebral edema or hydrocephalus result in increased intracranial pressure (ICP) when compensatory movements of the primary volumes have been exceeded. It has been shown in clinical studies that TBI patients with ICP greater than 20 mm Hg, particularly when refractory to treatment, have a worse prognosis and are more likely to have cerebral herniation syndromes. Cerebral perfusion pressure below 60-70 mm Hg, is associated with decreased cerebral parenchymal oxygenation altered metabolism and prognosis. The goal of neuromonitoring and treatment is at least maintaining cerebral perfusion, oxygenation and metabolism suitable, but also to limit the progression of elevated ICP, desaturation events.
ICP monitoring has been well documented to be an important predictor of prognosis in severe non-penetrating TBI as ICH is clearly associated with worse recovery and optimum control of elevated ICP leads to a better outcome. The available data suggest a higher frequency of raised ICP in CGI patients, and when present, raised ICP is documented to be a predictor of worse prognosis.35) In cases, where ICP is monitored and ICH is present, treatment measures are the same, which are used in non-penetrating TBI, i.e., hyperventilation, mannitol, CSF drainage, high-dose barbiturates, and more recently, decompressive craniectomy.245)
Surgical management
Surgical management of these patients is controversial. Some neurosurgeons favor a surgical approach consisting of minimal local debridement while preserving as much cerebral tissue as possible. Other neurosurgeons are more aggressive and try to remove all bone and any metallic fragments that are reasonably accessible.39) In theory, intracranial bone and metallic fragments that are not removed might be associated with a higher rate of infection, however in a small group of 13 patients, there was no correlation between the presence of retained fragments and the subsequent development of intracranial infection or epilepsy.37) In making a management decision, the neurosurgeon must take into account the type of weapon used and the distance from which it was fired, the patient's age and clinical condition and the CT scan findings. It is reasonable for the neurosurgeon to decide against active therapy for the patients in poor condition with multiple poor prognostic variables.59)
Tsuei et al.64) suggested an algorithm for penetrating gunshot injuries of the brain, in which according to GCS and pupillary reactivity, the decision to perform or not surgery is taken. Patients with a GCS 3 to 5 following resuscitation who have responsive pupils and are not hypotensive should have a CT scan;59) but those with GCS ≥3 and/or reactive pupils can undergo to head CT-scan, and based on findings, is decided to perform surgery or not (Figure 2).
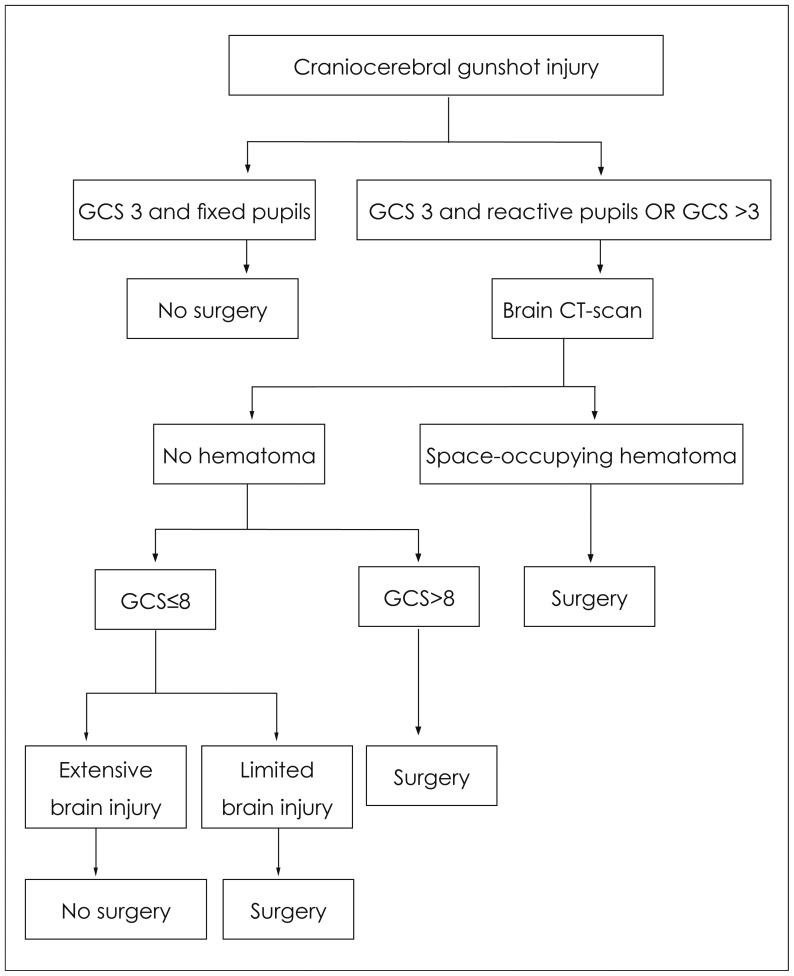 | FIGURE 2Management guideline for craniocerebral gunshot injury. Modified from Tsuei YS, Sun MH, Lee HD, Chiang MZ, Leu CH, Cheng WY, et al. Civilian gunshot wounds to the brain. J Chin Med Assoc 68:126-130, 2005.64) Copyright 2005 by the Elsevier. Reprinted with permission. GCS: Glasgow Coma Scale.
|
What to do on surgery?
Surgical procedures mainly included irrigation, debridement of devitalized tissues, and removal of space-occupying hematomas, in-driven bone, and accessible bullet fragments. For the treatment of CGI with small inlets the recommendation is local wound care and closure in patients without devitalized scalp and without significant intracranial pathologic findings. The term "significant" has not a clear definition, however, the volume and location of the hematoma, evidence of mass effect (midline shift >5 mm) or compression of the basal cisterns by edema or hematoma and the clinical condition of the patient, all belong to the term "significant".
The treatment of most extensive wounds with nonviable scalp or bone (significant fragmentation of the skull) is a large debridement with craniectomy or craniotomy before primary closure. In the presence of significant mass effect, debridement of necrotic tissue and secure access to the bone fragments is the recommendation, also hematoma evacuation (Figure 3). In the absence of significant mass effect, surgical debridement of projectile trajectory is not recommended on the basis of evidence Class III.52) Repairing of open sinuses with dural sealing is recommended, the clinical circumstances dictate the time of repair. The dural graft technique and the material used for closure are discretionary to the neurosurgeon.
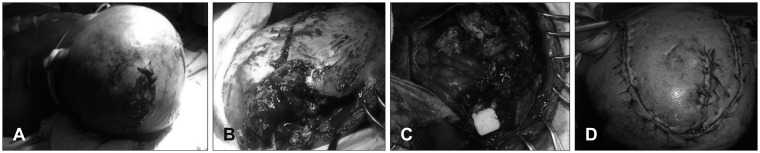 | FIGURE 3Adult male victim of craniocerebral gunshot injury (CGI) during assault. He was transferred promptly to our emergency service, received vigorous resuscitation despite Glasgow Coma Scale of 5 (E1V2M2) and emergent damage control neurosurgery. A: Image showing the inlet hole of CGI in left parietal region with perilesional tissue devitalization. B: Comminuted left skull associated to dural tear, brain laceration and bulging of macerated brain parenchyma. C: Postoperative image of subtotal left fronto-parietal lobectomy with drain of left intraparenchymal hemorrhage; hemisphere shows blunt damage and congestive feature. D: Suturing of operation site and inlet wound.
|
Regarding surgical management techniques, these vary whether civil literature and military literature were separately analyzed, especially for the following reasons:
1) The majority of injuries by gun fire in skull on the battlefield are produced by high-speed projectiles unlike most penetrating brain injuries in civilians.
2) Wounds are much more contaminated in the battlefield.
3) Early surgical treatment in the military is limited in comparison with the facilities of treatment on civilians.
4) The technical difficulties for adequate brain and cardiopulmonary resuscitation on the battlefield compared to the technical facilities in the civil situation.
Until the end of Vietnam War, was recommended the complete removal of metal and bone fragments, vigorous debridement and performing many surgeries as necessary to prevent complications such as infections, epilepsy and cerebral edema, but was demonstrated in prospective studies during wartime, that repeated craniotomies to remove retained fragments and vigorous exploration in the initial surgery exponentially increased the morbidity and mortality of these patients and their ineffectiveness in preventing seizures or infections, so the current trend is the realization of a less aggressive debridement.
The management of CSF fistulas should be early to prevent infections; regarding the choice of closure techniques and the material used is within the discretion of the neurosurgeon, although preferably autologous fascia lata graft can be recommended.
Regarding to performing craniotomy or craniectomy in patients with military injuries, the study of Rish et al.5657) is the most important, the standard protocol includes exposing the surgical field from the skull defect by craniectomy to the periphery, removing devitalized tissue, however, in this study there is no difference between the two groups in terms of morbidity (including postoperative infection) and mortality, in addition there was no ability to control the factors which initially led to the decision to perform craniotomy before craniectomy.
In terms of time to perform cranioplasty in military wounds the most representative study is from Hammon and Kempe, 26) the findings of the study were:
1) The incidence of post-cranioplasty complications was 56% in patients who had complications during the initial care (infection or CSF fistula).
2) Cranioplasty after 1 year of injury is recommended (post-cranioplasty complication 4% after 1 year vs. 20% within 1 year).
3) In patients without baseline complications there is no difference in infection rate or time of cranioplasty.
Go to :
Management of Complications
Vascular complications of CGI
As mentioned previously, angio-CT and/or conventional angiography may be considered to identify traumatic intracranial aneurysms (TICA) and arteriovenous fistulas in patients with SHW in orbitofacial or pterional region. Between 0.4% and 0.7% of all aneurysms are caused by trauma, approximately 20% of traumatic aneurysms are from penetrating traumas. The branches of the middle cerebral artery and the anterior cerebral artery are the most vulnerable to penetrating trauma, followed by the internal carotid artery. TICA should be suspected in patients with CGI, presenting with secondary neurological deterioration;23) are rare occurrences; the majority of these lesions develop in the anterior and middle cerebral artery distributions.30) TICA may appear as early as 2 hours post-injury, but also appear in a delayed fashion. TICA may regress, resolve, or grow with time; they are associated with intracranial hemorrhage in 80% of cases and subdural hematomas in 26% of cases; whenever possible, TICAs should be trapped and excised.30) The evolution of diagnostic neuroangiographic techniques provides opportunities for endovascular therapy of traumatic vascular lesions of the head and neck that are minimally invasive, attractive options in selected cases.15)
Management of CSF fistulas
During primary surgery all efforts should be directed to seal the dura to prevent CSF fistulas. Surgical correction is recommended for CSF fistulas do not close spontaneously or refractory to medical management. The management of fistulas in the inlet and outlet of the projectile require the closure of the dura mater, fascia and skin. Infection is the most common complication of penetrating brain injuries and is directly associated with increased morbidity and mortality,21) so prevention is essential to optimize their prognosis regardless of the initial management of the injury.
1) Retained fragments of bone or metal.
2) Time of surgery.
3) Use of antibiotics.
4) CSF fistulas.
In the study of Meirowsky et al.43) only 50% of the fistulas were at the site of entry or exit of the projectile, 72% occurred in the first 2 weeks of trauma and 44% closed spontaneously. The conclusion is that the more early CSF fistulas are treated less is the risk of infectious complications, morbidity and mortality.
Antibiotic prophylaxis in CGI
The use of broad spectrum antibiotics is recommended in patients with penetrating brain trauma.7) The risk of intracranial infection in patients with penetrating brain trauma is high due to the presence of foreign bodies, contaminated skin, hair and bone fragments in the path of the projectile. In this review we only make reference to antibiotic prophylaxis after trauma and before any clinical evidence of infection, management of established infection (wound infection, meningitis, brain abscess, etc.) are not discussed here.
The infection rate in the pre-antibiotic era during World War I as reported by Whitaker66) was 58.8% in the Second World War in the Post-Antibiotic Era in Slemon study compared the use of Sulfa Local and/or parenteral sulfonamide with an infection rate of 21% to 31%, but when added penicillin the infection rate dropped from 5.7% to 13%.63)
Regard bacteriological cultures there are few published studies, the most representative are those of Carey et al.10) in Vietnam reported that in 45% of the fragments removed mainly had positive cultures for gram-positive bacteria; in the study of Hagan25) in the Vietnam War Staphylococcus epidermidis was isolated; Aarabi1) in studying in the Iran-Iraq War of 1983-1984 found positive cultures in approximately 20% of cases, where were isolated staphylococcus, streptococcus and acinetobacter, and positive cultures in brain tissue removed for Staphylococcus, Acinetobacter, Escherichia coli, Klebsiella and Enterobacter.
Risk factors for infection, according to Arendall and Meirowsky4) are 29% for sinuses wound and 49% according to Meirowsky et al.43) for CSF fistulas. Regard to the use of antimicrobial agents as prophylaxis for penetrating brain trauma there is considerable variability, in a survey about Neurosurgical practice in the U.S. Kaufman34) reported that 87% of respondents neurosurgeons use cephalosporins, the 24% use chloramphenicol, 16% used penicillin, 12% used aminoglycosides and 6% vancomycin, less frequently were used erythromycin, miconazole and tetracyclines.
In patients who underwent surgery with removal of bullet fragments, wound debridement, and watertight dural closure, administration of prophylactic antibiotics was not associated with the incidence of intracranial infection secondary to penetrating cranial gunshot wounds. Projectile trajectory through potentially contaminating cavities, persistence of intraparenchymal osseous or metallic fragments after surgery, and prolonged hospital stay were independent risk factors for intracranial infection.31)
Anticonvulsive prophylaxis in CGI
Between 30 and 50% of patients with penetrating brain trauma develop seizures from 4 to 10% of them have their first seizure within the first week and 80% during the first 2 years, however, the risk decreases with time. Anticonvulsant medications in the first week after penetrating brain trauma are recommended to prevent early posttraumatic seizures (phenytoin, carbamazepine, valproic acid, and phenobarbital). Prophylactic treatment with anticonvulsants beyond the first week after penetrating brain trauma has not proven to prevent the development of new seizures and is not recommended.
Go to :
Mortality and Prognosis
With regard to mortality, exhibits devastating behavior, have been reported a mortality rate after penetrating craniocerebral injury varing from 23% to 92%, with higher mortality rates, approximately 87% to 100% in patients with low neurologic status on presentation.122344753) After surgical interventions mortality rates of CGI has been reported to be rounding the 20%8) in earlier studies and 7.4%41) to 18.7%51) in recent studies. Murano et al.46) identified the following variables as predictors of death: respiratory arrest on admission, hypotension on admission, transhemispheric and transventricular CGI.
As mentioned previously, one of the first challenges in managing patients with CGI is determining whether any intervention will result in an outcome that is acceptable to the patient, family, and society,16) in this circumstance, the postresuscitation GCS is the most reliable and significant clinical predictor of outcome to date.328405155) The series reported by Khan et al.36) confirmed the strong correlation between postresuscitation GCS score and outcome. Interestingly, they found no difference in outcome between penetrating (no exit) and perforating (entrance and exit) wounds. However, Joseph et al.32) found that survival rate increased incrementally over time to a rate of 46% with early aggressive resuscitation of all patients with gunshot wounds to the brain regardless of their presenting clinical picture, recommending that notion of low GCS should not deter the use of resources to treat and manage these patients.32) Other prognostic clinical factors include dilated, nonreactive pupils, hypotension, hypoxia, coagulopathy, suicide attempt, advanced age, and perforating wounds.13355255)
Go to :
Conclusion
There have been few recent studies involving penetrating craniocerebral injuries, and most studies have been restricted to small numbers of patients, which do not allow for adequate prediction of mortality. However, classic studies in military and civil environment have identified that this is a highly lethal or devastating violent condition, able to leave marked consequences for the affected individual, the family and the health system itself. Unfortunately this is a prevalent condition in developing countries, with major armed conflicts which is not very likely to achieve a high rate of prevention, since the main trigger is violence at the national or state level. Various measures have been aimed to lower the incidence of CGI, especially in civilians. It is important to recognize the role of vigorous and intense resuscitation but always evaluated together with predictors of mortality, to provide an individualized approach, especially because injuries from projectiles are different from each other, there is no equal. It is necessarily urgent to continue promoting research in a neurocritical topic such as CGI, looking impact positively the quality of life for those who survive.
Go to :
 XML Download
XML Download