

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The airplane is the preferred vessel for long distance transportation. Compared to car crashes, such incidences involving airplanes are relatively rare, yet airplane crashes are tragic disasters associated with much higher rates of injury and death.7)
Few studies examine spinal injuries in the context of airplane accidents. To the degree these studies exist, most of them are focused on cases of spinal injuries sustained during ejection from fighter jets, with most pilots experiencing thoracolumbar injuries.15810) These case series demonstrated that the injury mechanism and type of spine injury differ from those associated with motor vehicle accidents. On July 6, 2013, an Asiana Airlines flight from Seoul crashed during landing at San Francisco Airport (Figure 1). After initial conservative management, many of these patients were transferred to our hospital from San Francisco. Three of these patients had severe back pain immediately after the crash. These patients underwent evaluation, whereupon it was found that they had suffered compression fractures of the spine. In this report, we discuss the characteristics of the spine fractures and the mechanism of injury related with the airplane crash.
Case Report
Case 1
History and examination
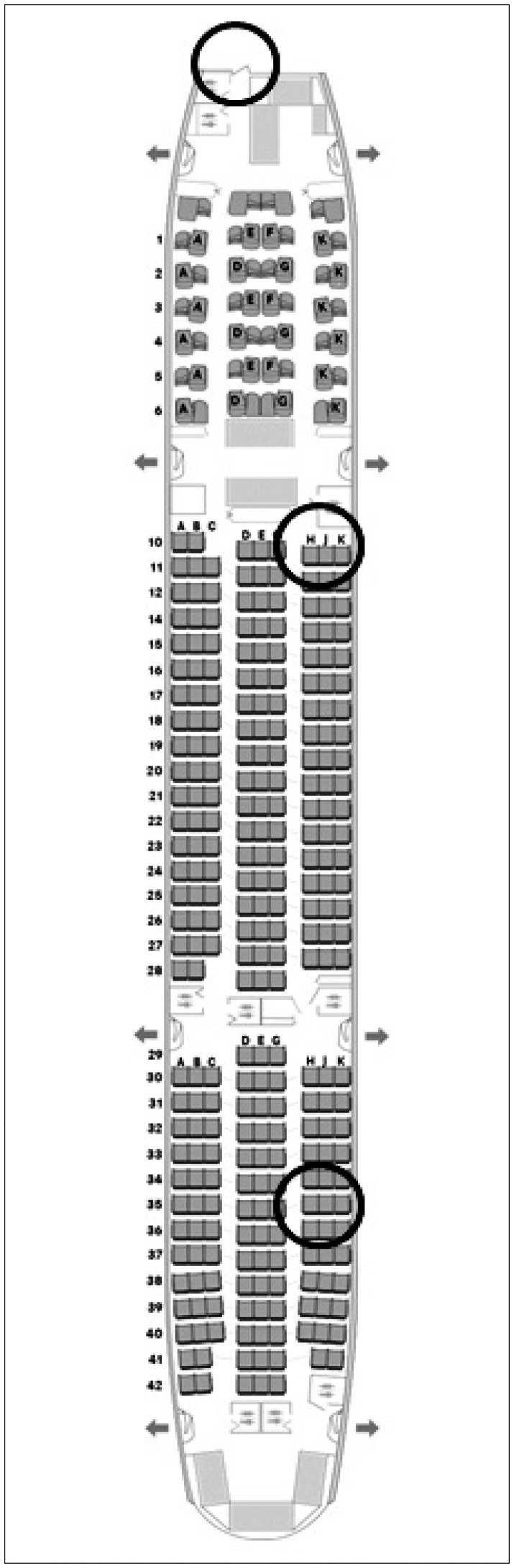
A 20-year-old woman sustained trauma during a plane crash. Her height and body weight measured 173 cm and 63 kg. She was seated in the rear of the aircraft (Figure 2). When the plane crashed, she was fastening her seatbelt, cradled head on seat front and feeling a lot of downward force. After the accident, she reported severe back pain without any other symptoms. On physical examination at our hospital, severe back pain was elicited with direct tenderness of the thoracic spine; a full neurological examination yielded normal findings without deficits.
Radiologic findings
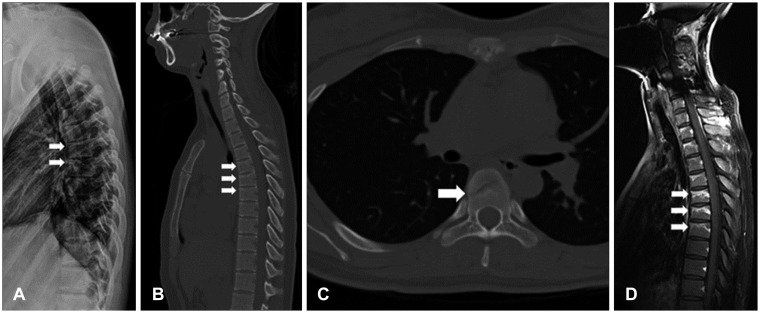
The X-ray showed compression fractures of the anterior upper portion of the T6 and T7 vertebral bodies (Figure 3A). Computed tomography (CT) images also showed fractures on the upper portion of the vertebral bodies and linear oblique fracture line in sagittal (Figure 3B) and axial (Figure 3C) images, respectively. Magnetic resonance imaging (MRI) was employed to look for evidence of spinal cord injury. T1 gadolinium-enhanced sagittal MRI showed multiple compression fractures of the upper thoracic level (Figure 3D) and no damage to the spinal cord.
Case 2
History and examination
A 33-year-old woman, measuring 170 cm tall and weighing 57 kg, was seated in the middle of the airplane (Figure 2). When the plane crashed, she reported feeling her body move in all directions with chest knee position, and afterward, an inflatable evacuation slide burst into the airplane and hit her. She lost consciousness, and then woke up with severe back pain. When she came to our hospital, she reported severe back pain, with pain elicited upon direct palpation of the lower back and left flank. Full neurological examination yielded no deficits.
Radiologic findings
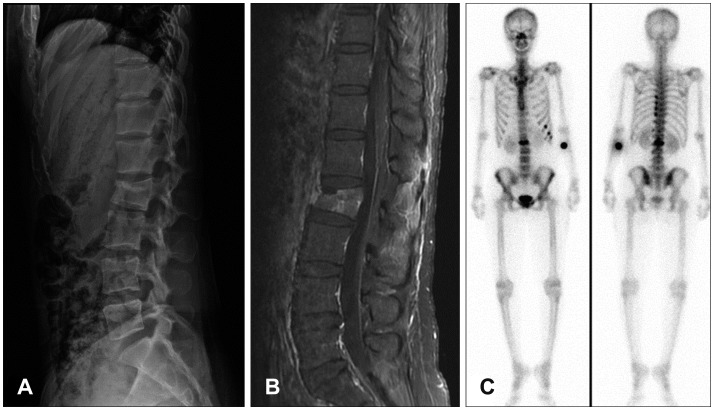
X-ray of the lumbar spine revealed anterior wedge compression fracture of the L2 vertebral body (Figure 4A), and MRI revealed a wedge compression fracture involving the middle column of the same vertebral body with posterior column signal change due to posterior ligament complex injury (Figure 4B). The wedge compression rate was approximately thirty percent. Whole body bone scan (Figure 4C) showed uptake at the L2 vertebral body and left 10th, 11th, and 12th ribs.
Case 3
History and examination
A 49-year-old man, standing at 170 cm tall and weighing 70 kg, was seated in the front of the airplane (Figure 2). The patient reported severe back pain after the accident with erected seated position, without other pain or any numbness. A full neurological examination yielded no deficits, and his back pain improved in a few days.
Radiologic findings
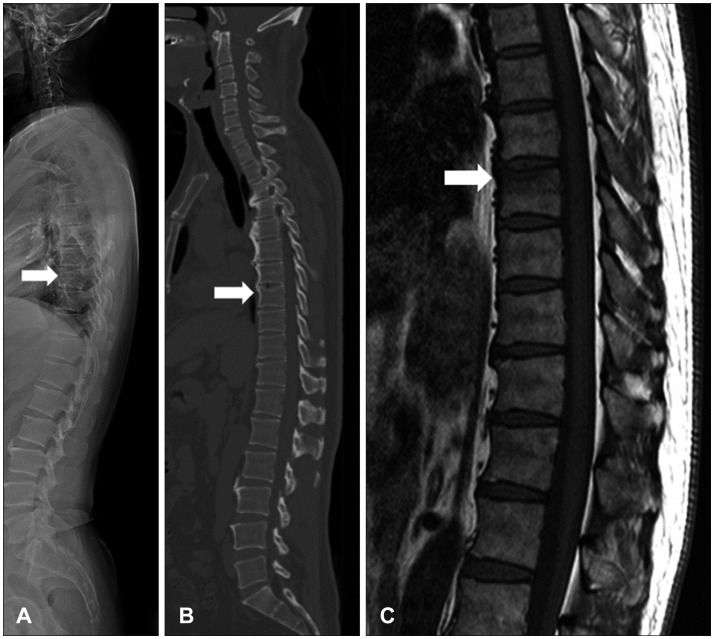
X-ray of the thoracic spine raised the suspicion of a compression fracture (Figure 5A). Similarly, sagittal CT images also pointed to a compression fracture of the T8 vertebral body (Figure 5B). T1 sagittal MRI revealed a wedge compression fracture of the anterior upper portion of the T8 vertebral body (Figure 5C).
Discussion
Crashes involving aircraft contribute greatly to injury and death statistics in transportation disasters. In the main, very few survive airplane accidents because high altitude crashes almost always occur with high speed or an explosion.3) In the rare event where many do survive a plane crash, the accident usually happens during take-off or landing. During these periods of the flight, the speed of the aircraft is slower than at any other point, thus the potential for many to survive exists, provided there is no second catastrophic event.269)
Spine fracture is an important and major injury of plane crash survivors. In reported cases, most survivors have spinal fracture, and spinal fractures are the second most common injury, following lower extremity fractures.
In the case of a plane crash in Iran in 2011, seventy-eight people were killed and twenty-seven people survived out of 105 passengers. Fifteen of the twenty-seven patients had fractures to their spine (Table 1). The types of spinal fracture included burst fracture (7 cases), compression fracture (5 cases), and fracture dislocation (3 cases). The most common level of injuries were the thoracolumbar junction (T10-L2, 13 cases) and mid thoracic level (2 cases).9)
In the case of an aircraft catastrophe in the Netherlands, 9 patients were killed out of 134 passengers. A total of 297 injuries were registered, with most of the injuries sustained to the head and face (81 cases), spine (31 cases), and extremities (34 cases). Of these injuries, 17% were spinal fractures.12)
In the case of a light airplane crash in Israel, one passenger out of six perished, with all 5 survivors having spine fractures. Those cases involved the thoracolumbar junction (3 cases), L4-5 level (1 case), and T6-7 level (1 case).1)
Ejection from the cockpit is another major cause of compression fracture associated with aviation disasters.11) Due to the high velocity gravity z-axis (Gz) force during ejection, the majority of these compression fractures involve the thoracolumbar junction. The thoracolumbar junction is a junction between thoracic kyphosis and lumbar lordosis, exhibiting hypermobility and hyperflexion during ejection or crash.4)
In our case series (Table 2), the second patient had an L2 compression fracture, which included the thoracolumbar junction, with posterior ligament complex injury. When the patient was injured, she was first subjected to a downward vertical force, followed by a strike to the body from a rapidly expanding inflatable evacuation slide. Despite the short interval between experiencing both forces as well as the different direction of the force vectors (Figure 6), the patient suffered a compression fracture. This finding suggests that the vertical Gz force was the primary traumatic vector. The mechanism of injury for this patient exhibits similarities to many other spine injury cases due to a plane crash, where thoracolumbar compression fractures were dominant.811) It may also have chance to have chance fracture for posterior ligament complex injury. Patient doesn't have definite contusion at seat belt area, but most of airplane's seat has a bar lap-only belts, especially in passenger seats, it may cause chance fracture.
The first and third cases in the present series were mid-thoracic level compression fractures without associated injuries. When these patients were injured, both reported feeling a strong, fast downward force, which we interpret as a high velocity vertical Gz force. And, as both patients only have compression fracture of the spine, we therefore concluded that the vertical Gz force was the major vector of the trauma. And we are also informed that few more patients are treated for compression fracture at other hospitals. Although automobile accidents have no the effect of Gz, airplane accidents can have the effect of Gz.
Survivors subjected to excessive vertical forces during an airplane crash are vulnerable to spine fracture. As such, survivors of aircraft disasters should undergo cautious and rigorous evaluation of the spine. Moreover, the design of airplane seats and seat belts should better incorporate protection from the vertical Gz force, in addition to the other directional forces.
Conclusion
Here we report three cases of spine fracture due to a commercial airplane accident in which 307 passengers were on board. Each of the three patients suffered compression fracture at the mid-thoracic and thoracolumbar junction. High velocity Gz force was the causative vector in all three patients. Therefore, the role of Gz force on spine injuries should be considered, and strategies to protect passengers from excessive Gz force during a plane crash should be developed.



 XML Download
XML Download