

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Break-dancing, a term named by a disc jockey in the South Bronx in New York City in the late 1970s, was first used to describe a style of street dance done to accompany the breakbeat, or syncopated rhythm, that disc jockeys used to set the pace for a piece of hip-hop music.6) The dancers are often called 'b-boys' or 'b-girls'. In contrast to the popularity of this sport, there were only case reports and small series dealing with injuries. Stress reactions and fractures of the spinal iliaca anterior superior, femur, carpal, metacarpal, and metatarsal bones, pulmonary embolism, Paget-Schroetter disease, ocular trauma, genitourinary injuries, and cervical injuries including fracture, slipped disc, and neurological deficit are reported.4) However, a systematic epidemiological study in break-dancers is rare.148)
According to an epidemiological study of musculoskeletal injuries in break-dancers in Korea,1) the incidence of musculoskeletal injuries were high; 95% of 42 study subjects experienced musculoskeletal injuries at more than one site and the most prevalent site of injuries were: wrist (69.0%), fingers (61.9%), and knee (61.9%).1) Another epidemiological study of 144 break-dancers,4) professionals had significantly more injuries and overuse syndromes than amateurs with significantly more injuries of the wrist, knee, hip/thigh, ankle/foot, and elbow, and break-dancing was considered as a potentially high-risk dancing sport.4)
Although the wrist was reported to be injured with high prevalence associated with break dancing, only the musculoskeletal injuries, such as sprain, strain, and tendinitis, were reported and no associate peripheral nerve injury was reported.1) This article reports an occurrence of the compression syndrome of the superficial sensory branch of the ulnar nerve, type III Guyon's canal syndrome in an amateur 'b boy' break dancer.
Go to : 
Case Report
A 23-year-old, right handed college man presented with a tenderness over the left hypothenar eminence and painful paresthesia over the ring and little fingers of 3 months duration. He trained himself as an amateur 'b boy' break-dancer without the supervised training for the last 10 months before presentation. The onset was gradual with repetitive training of several stylized movements including 'toprock', 'footwork', 'power moves', and 'freezes'. Upon development of left hand pain, he discontinued b-boying, however, the pain and paresthesia were not relieved. He had been treated with nonsteroidal anti-inflammatory drugs (NSAIDs) and physical therapy under the clinical diagnosis of wrist sprain for two months, however, his symptoms were not relieved.
On physical examination, tenderness was noted over the hypothenar eminence. Digital pressure over the hypothenar eminence elicited a paresthesia over left ring and little fingers. There was no weakness on finger nor limitation of wrist motion. No hypesthesia or allodynia was observed except paresthesia. There was no evidence of fracture or deformity in the X-ray films of left hand. The magnetic resonance imaging (MRI) of the left hand showed minimal swelling the ulnar nerve with subtle enhancement within the Guyon's canal without soft tissue swelling (Figure 1). Mild effusion of the intercarpal and carpo-metacarpal joint was noticed as a traumatic change. The sensory nerve conduction study demonstrated decreased amplitude of sensory nerve action potential (SNAP) in the left ulnar nerve with abnormality of the motor nerve conduction and electromyographic examination.
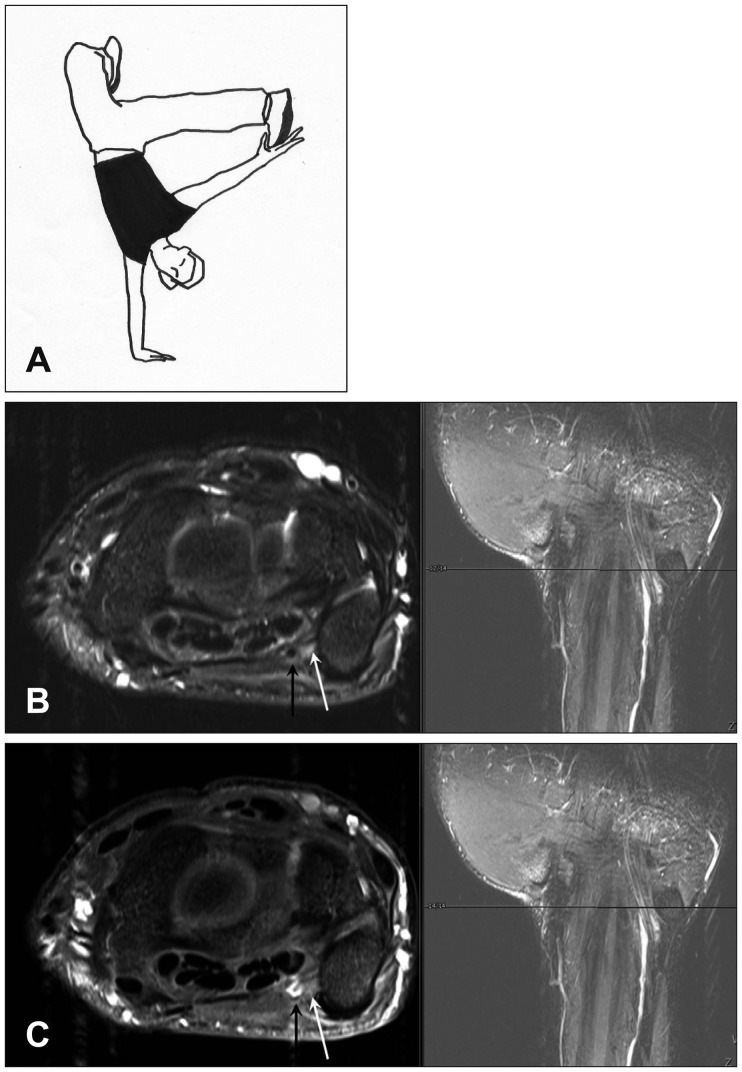 | FIGURE 1Break-dance posture and magnetic resonance imaging findings of type III Guyon's canal syndrome. A photograph showing a 'freeze', one of several stereotypical movements of break-dance which might be stressful to the wrist (A). T2-weighted axial (B) and fat-suppressed T1-weighted axial images (C) of the Guyon's canal showing the ulnar nerve (white arrow) and the ulnar artery (black arrow). There was subtle enhancement of the ulnar nerve. Note right side, the T2 coronal images taken from the scout images corresponding the level of axial images.
|
With the clinical symptoms and signs of tenderness and the distribution of paresthesia, combined with a decreased SNAP with preserved motor conduction on nerve conduction velocity examination along with the MRI findings, a diagnosis of type III ulnar tunnel syndrome (Guyon's canal syndrome) was made. An exploration of the Guyon's canal for decompression of the superficial branch of the ulnar nerve was planned after an additional course of medical treatment including corticosteroid (hydrocortisone 20 mg) with NSAIDs for 4 weeks. Month after medical treatment, the patient's pain and paresthesia were significantly alleviated and further observation with discontinuation of the medication was followed. He was free from pain and paresthesia after two months of observation.
Go to :
Discussion
Break-dancing reached the height of its popularity in the early and mid-1980s, faded away for a while, and then became popular again in the 1990s. The widespread public use of the Internet starting in the late 1990s gave break-dancers a new venue for acquiring a wider audience.1) Under the influence of internet, dance was popularized around world, and an entire sub-branches has evolve around it.1) Although there has been the reports regarding the injuries in ballet dancers, modern dancers, and theatrical dancers, an epidemiological study in break-dancers is relatively rare.148)
According to Kauther et al.,4) professional break dancers was reported to have significantly more injuries and overuse syndromes with injuries of the wrist, knee, hip/thigh, ankle/foot, and elbow. No significant differences were found in the time lost per injury and the time lost per overuse syndrome. Other recent, Korean epidemiological study by Cho et al.1) showed that 95.2% of break-dancers suffer from the musculoskeletal injuries at more than one site and the wrist was the most prevalent site of injury. According to Cho et al.'s study,1) the rate of injuries was significantly higher in amateurs without supervised training than professionals, and they stressed out the importance of careful screening, instruction and supervised training to prevent injuries.
The musculoskeletal injuries that have far been reported in break-dancers include sprain; strains; tendinitis; bursitis; growth plate injuries; fractures of the clavicle, radius, ulnar, carpal bone; phalanx and fifth metatarsal bone; stress fractures of the femur and calcaneus; vertebral fractures; and spinal cord injuries.12) And the most common type of injuries are sprain, strain and tendinitis, otherwise peripheral nerve injuries are rarely reported. It seems that several basic stylized movements including 'toprock', 'uprock', and 'freeze' would cause a serious burden and stress to multiple joints, especially in the wrist.
Guyon's canal, or the ulnar-carpal canal refers to the ulnar tunnel at the wrist named for the French surgeon Jean Casimir Félix Guyon, who described this space in 1861.5) The canal is composed of medially pisiform bone and laterally hamate's hook. The roof of Guyon's canal is formed by palmar carpal ligament and the floor is formed by transverse carpal ligament. Guyon's canal is approximately 4 cm long, from proximal edge of transverse carpal ligament to the aponeurotic arch of hypothenar muscles, and it contains ulnar artery and ulnar nerve.
When ulnar nerve runs through the aponeurotic arch of hypothenar muscles, it divided into two branches, superficial sensory branch and deep motor branch, and distal ulnar nerve lesions are classified into one of three categories.3) Type I Guyon's canal syndrome shows motor weakness of ulnar innervated muscle and sensory loss in the palmar surfaces of the hypothenar eminence and the fourth and fifth fingers, because it is related to the compression of proximal part of Guyon's canal. Type II Guyon's canal syndrome, compression of the deep motor branch, leads to the weakness of ulnar innervated muscle and spares sensation. Type III Guyon's canal syndrome only involve sensory loss in the little finger's palmar surface and the ring finger's ulnar side and spares motor, and our case is related to type III with this classification (Figure 2).
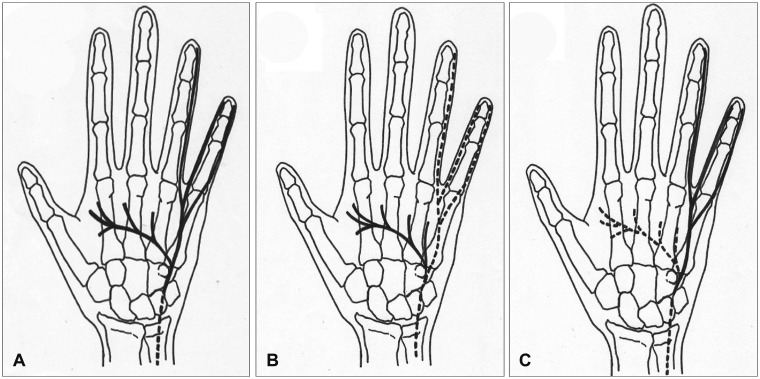 | FIGURE 2Schematic drawings showing the anatomical differences, depending on the types of Guyon's canal syndromes. A: Type I Guyon's canal syndrome, which is related to the compression of proximal part of Guyon's canal, that causes motor weakness of ulnar innervated muscle and sensory loss in the palmar surfaces of the hypothenar eminence and the fourth and fifth fingers. B: Type II Guyon's canal syndrome, results from the compression of the deep motor branch, leads to the weakness of ulnar innervated muscle and spares sensation. C: Type III Guyon's canal syndrome, only causes sensory loss in the little finger's palmar surface and the ring finger's ulnar side and spares motor (bold full line: the potential site of injuries to the ulnar nerve and its distal symptomatic branches).
|
Conservative treatment remains the first line in treating ulnar nerve compression in the Guyon's canal syndrome.7) Avoidance of repetitive trauma, rest immobilization (splinting), local corticosteroid injection, and anti-inflammatory medication may be tried individually and in combination to achieve relief. Any underlying disease leading to nerve damage must be treated. To prevent permanent nerve damage, surgical decompression of the ulnar nerve is recommended if there is no relief of symptoms within 6 months or development of muscle atrophy or weakness.7)
Go to :
 XML Download
XML Download