

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Infantile posthemorrhagic hydrocephalus (IPHH) is defined as ventricular dilatation after germinal matrix (GM) hemorrhage in a preterm infant. The GM is a gelatinous, highly cellular, and vascularized structure located near the head of the caudate nucleus, just beneath the ependymal lining. This structure develops to its maximal size by 23 weeks of gestation and involutes by 36 weeks.1581017) Preterm infants have a high risk of GM hemorrhage because of exposure of the fragile and immature vessels in the GM to stressful conditions, such as blood pressure fluctuations, increased cerebral perfusion pressure, and coagulopathy.1720) Dilatation of the ventricle occurs by alterations of cerebrospinal fluid (CSF) circulation resulting from GM hemorrhage into the ventricle.
Although the incidence of GM hemorrhage in preterm infants has decreased because of advances in neonatal care, the rate of GM hemorrhage is still as high as 30%.1213) Furthermore, the incidence of GM hemorrhage increases with decreasing birth weight. Temporary neurosurgical procedures for hydrocephalus include lumbar puncture, ventricular tap, external ventricular drainage (EVD), ventricular access device, and placement of a ventricular subgaleal shunt. Placement of a ventriculo-peritoneal (VP) shunt, which is a permanent procedure, is required in cases where CSF circulation fails to be restored. However, because there are many complications associated with invasive procedures, such as infection, ventricular isolation by infection, CSF leakage, shunt malfunction, over-drainage, and skin breakdown over the shunt device, meticulous procedures are required for these patients.23) Here, we describe our experience of the treatment and discuss the results of six IPHH patients treated by a VP shunt.
Go to : 
Materials and Methods
Between April 2010 and December 2014, six preterm infants had a VP shunt placed due to GM hemorrhage and hydrocephalus at our institution. Medical records and radiographic findings were analyzed retrospectively. All patients in the neonatal intensive care unit were scanned by cranial ultrasonography (USG) at the first 2 days of life and thereafter every week. GM hemorrhage and ventricle dilatation on USG were classified according to the Papile classification.15) Ventricle dilatation was estimated by the ventricular index (VI), which is the distance between the falx and lateral wall of the anterior horn in the coronal plane at the level of the third ventricle.2) Computed tomography (CT) was performed to evaluate the posterior fossa and to confirm the trajectory and the length of the intracranial catheter before VP shunt placement. EVD was performed in patients with symptomatic ventricular dilatation. The placement of EVD was maintained for 1 week and about 20 cc of CSF was drained per day. After serial rounds of USG, a VP shunt was placed in cases where there was no improvement in VI despite several rounds of EVD, no evidence of CSF infection, and patient weight over 1,500 g. In the operating room, we inserted an intracranial shunt catheter along the axis of the lateral ventricle via the occipito-parietal point. Other VP shunt procedures were performed in a routine fashion with a programmable valve. In one case with multiloculated hydrocephalus confirmed by preoperative imaging findings, we used a neuroendoscope for fenestration of the pseudomembrane, septum pellucidum, and Sylvius aqueduct. Patient symptoms, such as neurodevelopmental delay, seizure, and cerebral palsy, were evaluated as neurological outcomes.
Go to :
Results
Clinical data (gender, gestational age, weight at birth, VI, Papile grade, weight at VP shunt placement, associated problems) and surgical outcomes (time from birth to EVD, number of times EVD, time from EVD to VP shunt placement, complications of EVD, neuroendoscopic procedures, complications of shunt, final neurological deficits) are summarized in Tables 1 and 2. VP Shunt was placed in six patients after the diagnosis of IPHH. Four patients were male (66.7%) and two were female (33.3%). Mean gestational age was 25 weeks (range, 22 to 27 weeks) and mean weight at birth was 868.3 g (range, 450 to 1,140 g). Mean VI was 19 mm (range, 14 to 23 mm), and the VI of all patients was over the 97th centile. One patient (16.7%) had a Papile grade II hemorrhage, three patients had a grade III hemorrhage (50%), and two patients had a grade IV hemorrhage (33.3%). Mean weight at VP shunt surgery was 1,988.3 g (range, 1,700 to 2,500 g). Three patients had an isolated 4th ventricle.
The mean number of EVD sessions was 2.8 (range, 1 to 4) and the mean time from EVD to VP shunt placement was 38.3 days (range, 10 to 57 days). EVD complications occurred in two patients: one case of ventriculitis and one case of a ventricular abscess. Neuroendoscopic procedures were done in two patients: one patient underwent fenestration of the pseudomembrane while the other underwent fenestration of the pseudomembrane and septum pellucidum as well as aqueductoplasty due to multiloculated hydrocephalus. VP shunt complications (occlusion of the intracranial catheter) occurred in two patients (33.3%). Three of six patients had severe neurodevelopmental delay, two had mild neurodevelopmental delay, and one showed a normal development status at the end of the study. There was no mortality and no shunt infection.
Illustrative cases
Case 1 (patient No. 2)
The patient was born at 25 weeks gestational age by normal spontaneous vaginal delivery in our hospital. The patient was male and weighted 830 g. GM hemorrhage on USG was diagnosed 7 days after birth and classified as Papile grade III (Figure 1A). The patient was stable, but the fontanel became tenser and the head circumference increased after 84 days. We performed one round of EVD and the raised intracranial pressure (ICP) went down. Although the EVD was kept for 1 week, the fontanel became progressively tenser at 2 days after removal of EVD. We therefore placed a VP shunt; the patient's weight was 2,500 g at the time of this procedure. After 6 months, the patient suffered from sudden onset of nausea, vomiting, and lethargy. A CT scan revealed severe ventricular dilatation. We inserted a neuroendoscope via the previous intracranial catheter insertion site. Neuroendoscopic findings were an intracranial catheter encased by the choroid plexus (Figure 1B). We coagulated and detached the choroid plexus from the intracranial catheter using the neuroendoscope, and replaced the intracranial catheter with a new one. At the last follow-up at 49 months, the patient had a normal neurological status.
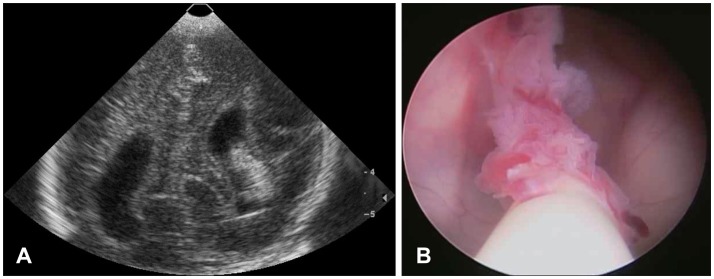 | FIGURE 1A case with complicated by proximal catheter occlusion. A: Ultrasonography taken seven days after birth shows intraventricular hemorrhage with dilatation of the lateral ventricle. B: Intraoperative neuroendoscopic view at the time of shunt revision shows encasement of choroid plexus around the intracranial catheter.
|
Case 2 (patient No. 5)
The male patient was born by Cesarean delivery at 23 weeks gestational age. His weight was 760 g. He had a Papile grade III GM hemorrhage based on USG at 14 days after birth. The patient presented with bulging of the fontanel and a lethargic status after 1 week. He underwent four rounds of EVD because ventricular dilatation did not resolve. His weight was less than 1,500 g. The patient developed severe ventriculitis (ventricular abscess) due to repeated EVD. Although the ventriculitis recovered and his weight increased to over 1,500 g (2,120 g) after 54 days, CT demonstrated multiloculated hydrocephalus (compartmentalization of lateral, 3rd, and 4th ventricles) (Figure 2A and B). We performed fenestration of the pseudomembrane of the multiloculated lateral ventricle and septum pellucidum, and facilitated communication between the 3rd and 4th ventricle (aqueductoplasty). We also placed a VP shunt. The following CT scan showed dilatation of the 4th and lateral ventricles after 8 months. We identified occlusion of the intracranial catheter due to encasement by a pseudomembrane and obstruction of the Sylvius aqueduct based on a neuroendoscopic view. We therefore inserted a stent (shunt catheter) into the Sylvius aqueduct and placed an additional VP shunt (Figure 2C and D). The patient showed severe neurodevelopmental delay and seizures at his last follow-up at 27 months.
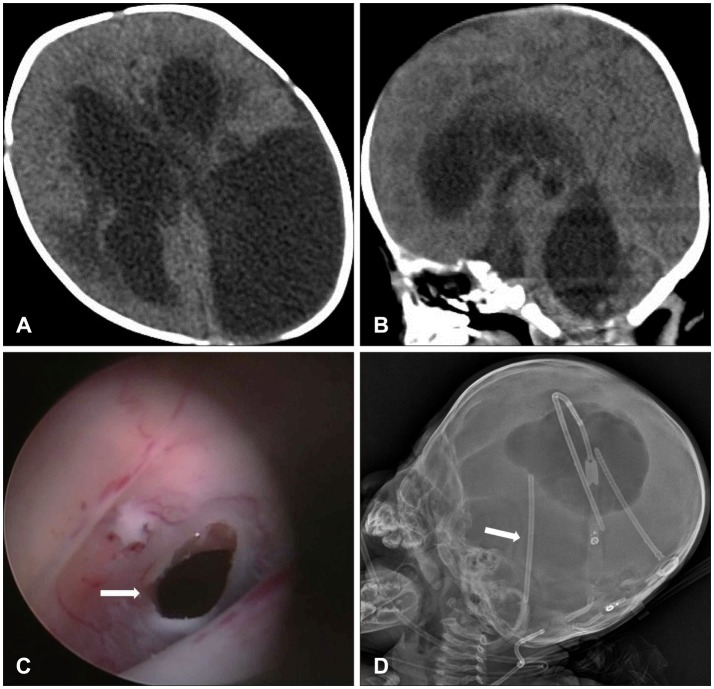 | FIGURE 2A case complicated by multiloculated ventricle. Multiple septations of lateral, 3rd, and 4th ventricle is shown in computed tomography (A, B). Sylvius aqueduct was reopened by a neuroendoscope (white arrow in C), and stent insertion into the Sylvius aqueduct is shown on the skull X-ray (white arrow in D).
|
Go to :
Discussion
Temporary surgical procedures can be performed to divert CSF from hydrocephalus to prevent brain tissue damage from raised ICP and to avoid placement of a permanent shunt.22) These procedures include lumbar puncture, ventricular tap, EVD, insertion of a ventricular access device, and insertion of a ventricular subgaleal shunt. However, previous studies have reported that the incidence of shunt dependency and complications (infection) are 65% and 60%, respectively. EVD with continuous CSF drainage is an effective procedure.49) We performed the procedure by inserting an intravascular catheter (20 gauge) via an unclosed coronal suture in the neonatal intensive care unit, not the operating room. This is a simple and safe procedure, but the rate of infection was 33.3% (two of six patients) in our study. In these two patients with infection, EVD was performed four times each, while it was performed less than four times in three other patients and four times in the last patient. Six patients was underwent EVD and all six patients had a VP shunt placed. Therefore there was no shunt independence by EVD.
Multiloculated hydrocephalus refers to intraventricular septa formation due to subependymal inflammatory gliosis and formation of intraventricular deposits.14) Ventricular infection increases the incidence of multiloculated hydrocephalus. In particular, an isolated 4th ventricle is identified by compartmentalization of only the 4th ventricle due to blockage of the Sylvius aqueduct and foramina of Magendie and Luschka by subependymal gliosis and arachnoid scarring. Fourth ventricle is dilated by CSF produced by the choroid plexus. Clinical symptoms, such as ataxia, apnea, and swallowing difficulty, are induced by brain stem compression. Treatment options for isolated 4th ventricle are VP shunt placement or communication between the 3rd and 4th ventricles (aqueductoplasty) using neuroendoscopic techniques. If the Sylvius aqueduct is obstructed again despite aqueductoplasty, stent insertion in the Sylvius aqueduct is effective compared to aqueductoplasty alone.3) We had three cases with an isolated 4th ventricle. Two cases developed after ventricular infection while there was no evidence of infection in the third case. Two cases had a VP shunt placed, while the other underwent aqueductoplasty using a neuroendoscope. In the case in which aqueductoplasty was performed, the Sylvius aqueduct was obstructed again after 8 months, so we inserted a stent into the Sylvius aqueduct using a neuroendoscope. No complications associated with stent insertion were observed at the last follow-up.
Generally, neurodevelopmental outcome of IPHH is determined by the grade of GM hemorrhage, coexistent parenchymal injury, and progression of ventriculomegaly.1819) Patients can suffer mental retardation, seizure, and cerebral palsy. The timing of GM hemorrhage is an important factor that affects neurodevelopmental outcome. Especially, patients who develop GM hemorrhage within 6 hours of birth have a poor neurodevelopmental outcome.19) Progression of ventricular dilatation and signs of raised ICP are also important factors to consider. A patient who develops ventricular dilatation without symptoms related raised ICP has a more favorable prognosis than symptomatic patients.6) Three of our patients had severe neurodevelopmental delays and seizures. The mean Papile grade of these three patients was 3.6, while the mean Papile grade of the other three patients was 2.6. Although we could not evaluate the significance of this result because of the small number of patients, Papile grade could affect neurodevelopmental outcome. However, because two of three patients with severe neurodevelopmental delay also had ventricular infection, we could not verify that Papile grade is an important factor affecting neurodevelopmental outcome. A large number of patients and multivariate analysis will be necessary to test this hypothesis.
A VP shunt is the traditional CSF diversion treatment for hydrocephalus. However, it has many complications, such as infection, CSF leakage, disconnection, shunt malfunction, over-drainage, and skin breakdown over the shunt device. Because preterm infants have immature immune systems, infection associated with the shunt device as a foreign body develops frequently. Furthermore, skin breakdown due to a thin scalp and scalp thinning associated with increasing head size may occur.11) Endoscopic third ventriculostomy (ETV) is usually performed for noncommunicating hydrocephalus of children older than 2 years. ETV had not been considered as a treatment modality for IPHH. However, studies about effectiveness of ETV have been reported recently as a treatment option for hydrocephalus of IPHH.16) And there were reports addressing medical treatments and alternative temporary surgical procedures (ventricular access device and ventriculosubgaleal shunt insertion) to reduce a rate of complication.1321) We placed a VP shunt in all IPHH patients. No shunt-associated complications except for occlusion in two patients occurred in our study.
One patient (patient No. 2) had an excellent neurodevelopmental outcome as evidenced by normal cognitive function, no developmental delay, no seizures, and no cerebral palsy. Despite a GM hemorrhage and ventricular dilatation of Papile grade III, symptoms and signs associated with raised ICP were not observed for 84 days. Gestational age, weight at birth, VI, and Papile grade were not different from those of the other patients, so these cannot be considered to be factors associated with a good outcome. Delayed symptom development may be an important factor that affects neurodevelopmental outcome. Because late developing symptoms are associated with fewer EVD procedures, there is less chance of EVD complications, and the rate of infection and VP shunt complications are likely to be lower. However, more cases need to be examined to confirm this hypothesis.
Go to :
Conclusion
In our study, although it is difficult to present the significant result for management of IPHH because of the small number of patients, we think that varied efforts associated with neonatal intensive care, meticulous procedures, and less invasive operations are required to treat IPHH patients who are in poor condition and generally have a high rate of complications. A large number of patients and long-term follow-up are required to determine factors that affect neurodevelopmental outcome.
Go to :
 XML Download
XML Download