

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Decompressive craniectomy (DC) is performed in medically refractory situations involving elevated intracranial pressure (ICP), such as intracerebral bleeding, traumatic brain injury (TBI), and ischemic brain lesion leading to severe brain swelling.517) Cranioplasty is then performed for cosmetic, protective and physiologic reasons after the cerebral edema has resolved.467) Cranioplasty itself is known to have a higher postoperative complication rate than other elective cranial procedures, such as wound infection or dehiscence, intracranial hematoma, and sunken bone flap and seizure.2922) Bone flap resorption (BFR), one of the long-term complications of cranioplasty, can result in structural breakdown.121421) Because BFR requires reoperation and replacement of the flap with plastic, metal, or other materials, investigation of the frequency of BFR and the associated risk factors is needed. The purposes of this study were to carry out such an investigation, along with a review of the literature, and to suggest optimal strategies for improving prognosis of patients who require cranioplasty.
Go to : 
Materials and Methods
Definition of BFR
Cosmetic disfigurement was the main complaint in patients diagnosed with BFR. We defined BFR as complete or partial resorption of the bone flap covering a lesion of diameter >1 cm, where the remnant thickness of the bone flap was less than 50% of that of the contralateral region of the skull (Figure 1).
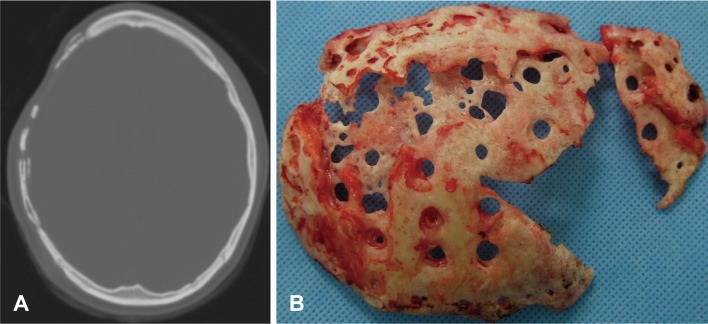 | FIGURE 1A: Computed tomographic image of bone flap resorption demonstrating partial resorption of the bone flap, where the remnant bone flap was less than 50% as thick as the contralateral region of the skull. B: Photograph showing bone flap resorption. The multiple holes in the bone flap are thought to have been made for epidural tack-up suturing in the preceding cranioplasty. Such holes may expand as bone resorption progresses, causing cosmetic problems.
|
Patients
From October 2003 to December 2012, 162 patients underwent cranioplasty after DC in our institution, and were followed up for at least a year. The DC was performed for intractably elevated ICP occurring despite medical treatment in an acute situation, or during the course of intensive care. We performed a retrospective chart review examining demographic data, diagnosis, time interval between DC and cranioplasty, and number of major cranial operations before cranioplasty. Major cranial operations were defined as operations that needed craniotomy in which a bone flap was taken. We included patients where the cranioplasty was performed to repair skull defects after DC, and excluded patients where it was performed for other reasons such as reconstruction of a depressed skull fracture. Initial diagnoses were classified in 5 categories; 1) TBI, 2) cerebral infarction, 3) subarachnoid hemorrhage (SAH), 4) intracerebral hemorrhage (ICH), and 5) others.
Bone flap preservation
Connective tissue such as pericranium, muscle, fascia, and galea on the bone flap was removed after the bone flap was obtained. Then the cleaned bone flap was dried in an Amsco® Warming Cabinet (STERIS Corporation, Mentor, OH, USA) at 110-120℃ for 1-2 days. After drying it was sterilized at 70℃ for 75 minutes with a Sterrad® NX™ Sterilization System (Advanced Sterilization Products, Irvine, CA, USA) that exploits hydrogen peroxide and low temperature gas plasma. After sterilization, the flap was kept aseptically at room temperature, and resterilized twice more in the same manner, one and two days before the planned cranioplasty.
Operative procedure
The subsequent cranioplasty was scheduled by the surgeon after resolution of the brain edema, taking into account the patient's neurological status, of course, and also various other factors including the patient's general medical condition and economic status.
Under general anesthesia, the cutis and subcutis were opened along the previous incisions and dissected from the cranium and the temporal muscle. After trephination of multiple holes for epidural tack-up suturing in the flap, it was fixed in its original position, contacting the edge of the bone defect as closely as possible with titanium plates and screws. The temporal muscle, if preserved, was separated from the dura mater and fixed onto the bone flap. Epidural and subcutaneous drains were inserted before wound closure, and antibiotics were administered intravenously for 7 days after the cranioplasty.
Statistical analysis
We performed a logistic-regression analysis to identify risk factor for BFR. To solve the problem of multicollinearity due to closely correlated variables, we calculated variance inflation factors (VIFs) and excluded variables with VIFs >10. Thereafter variables were selected by backward elimination.
Go to :
Results
Patient characteristics
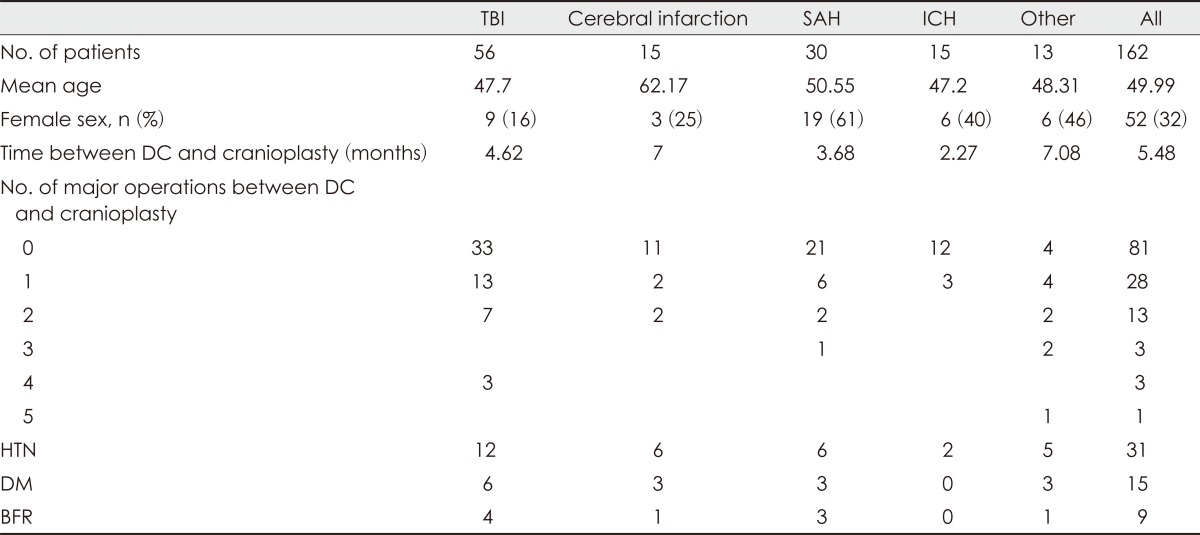
Of the 162 patients who underwent cranioplasty, 110 were male and 52 female. Patient age ranged from 13 to 85 years (mean, 49.99 years), and the time interval between DC and cranioplasty varied from 29 days to 10 years (mean, 5.48 months). We categorized 129 patients according to the number of major cranial operation undergone before cranioplasty: 81 had no major cranial operation before cranioplasty, 28 had 1 operation, 13 had 2 operations, 3 had 3 operations, another 3 patients had 4 operations, and 1 patient had 5 operations. The other 33 patients from whose medical records this information had been omitted were excluded.
We also categorized the patients by their initial diagnosis: 56 cranioplasties were performed in patients with TBI, 15 in patients with cerebral infarction, 30 in patients with SAH, 15 in patients with ICH, and 13 in patients with other diagnoses. BFR occurred in 4 patients with TBI, 1 with cerebral infarction, 3 with SAH, and 1 patient with some other diagnosis. Patient characteristics at initial diagnosis are shown in (Table 1).
Risk factors for BFR
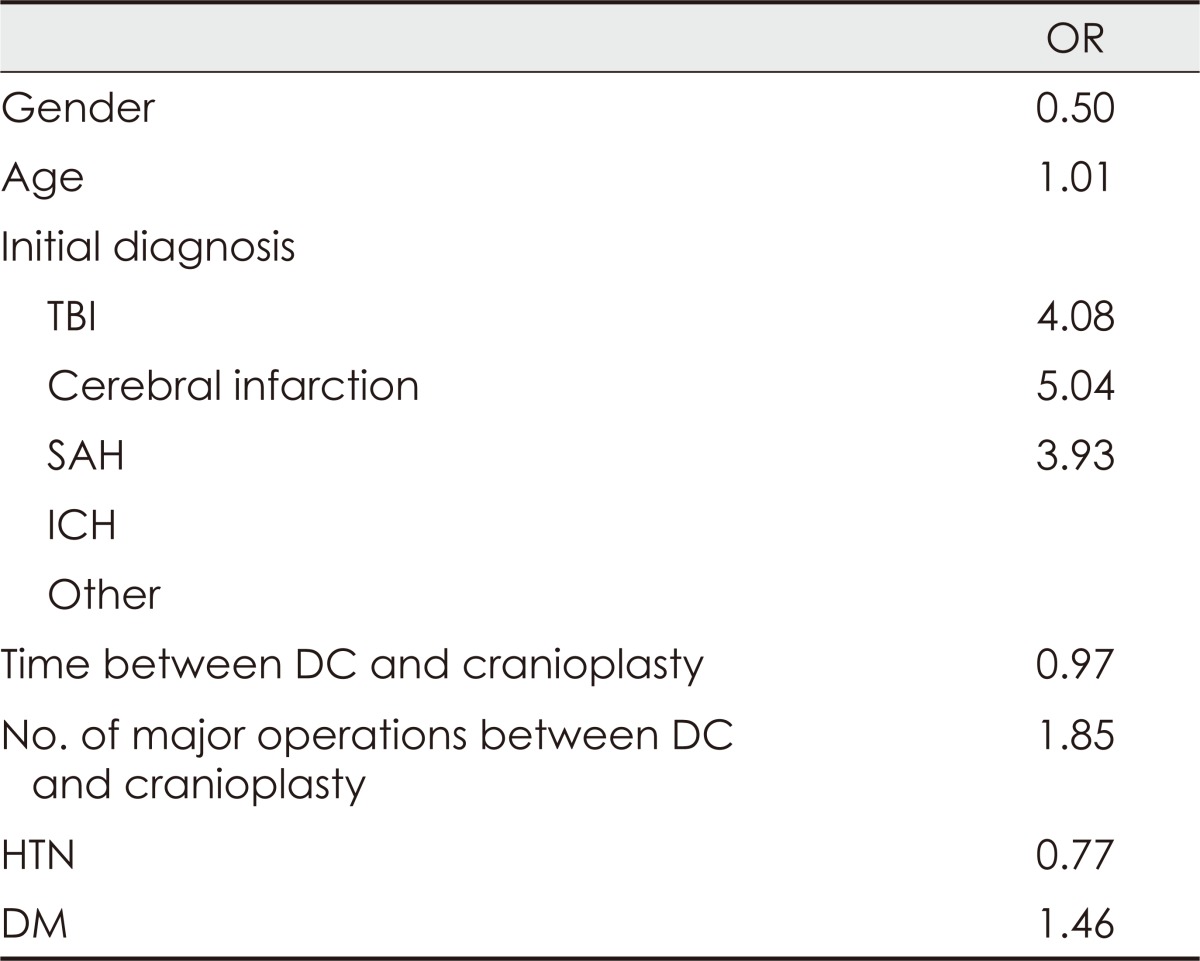
No variable was significantly associated with BFR in the logistic-regression analysis. This may have been primarily due to the small BFR sample size. However, there was a relative risk according to initial diagnosis: cerebral infarction [odds ratio (OR) 5.04], TBI (OR 4.08), and SAH (OR 3.93). Table 2 presents the results of the logistic-regression analysis.
Go to :
Discussion
DC is the standard surgical option for malignant cerebral edema resulting from intracranial hemorrhage, cerebral infarction and TBI.517) After the cerebral swelling has resolved, cranioplasty is then performed to correct the skull defect. This is not just a cosmetic measure, since it also provides important support, and restores normal cerebrospinal fluid flow, reducing the formation of pseudomeningoceles and protecting vital structures.67) Because almost all patients surviving a DC require cranioplasty, the complications of this second operation need to be acknowledged. Cranioplasty always carries the risk of complications, especially as the patients are often weakened by the impact of the first event that required DC. BFR is one of the known long-term complications of cranioplasty following DC. It has been reported in 7.2-50% of cases.91011141621)
Survival of a bone implant is acknowledged to depend on the reaction of the surrounding tissue and on functional contact between the cancellous bone and adjacent resident bone.20) According to Kalfas,15) it is crucial that inflammation and revascularization occur in the first 1 to 2 weeks for bone graft healing. The incorporation and remodeling of a bone graft require that mesenchymal cells have vascular access to the graft in order to differentiate into osteoblasts and osteoclasts.15) Osteoinduction refers to the process by which primitive mesenchymal cells differentiate into osteoprogenitor cells. These latter then differentiate into osteoblasts that can form new bone to replace the necrotic bone, which is gradually absorbed. Osteoprogenitor cells from the surrounding tissue migrate into the three-dimensional structure of bony and protein matrix in a process called osteoconduction. It is now understood that auto- and allo-grafts rely on osteoconduction as the main mechanism underlying cranioplasty.20) As healing progresses, the bone graft is remodeled through resorption of necrotic bone and formation of new bone. We believe that BFR may occur due to dysregulation of osteoconduction.
We failed to identify any variable significantly associated with BFR. However, there was a relative risk with TBI and cerebral infarction as initial diagnosis. The risk of BFR was 5-fold greater in patients with cerebral infarction than in those without cerebral infarction, and 4-fold greater in those with TBI than in those without TBI. There has been no study, to our knowledge, of the relationship between cerebral infarction and BFR. We suggest that atherosclerotic changes due to poor microcirculation in ischemic stroke patients may inhibit revascularization in the bone healing process. On the other hand there are some studies concerned with the relationship between BFR and TBI. According to Schuss et al.,21) BFR occurs significantly more often in patients who undergo DC for TBI than in those undergoing DC because of any other primary diagnosis (8.5% vs. 1.8%). They also found that BFR was more frequent in patients with multiple fractures or fragments in the reinserted bone flap than in those without such multiple fractures or fragments (17.2% vs. 2.2%).21) We suppose that the larger surface area of bony fragments accompanying multiple fractures make bone proteins more susceptible to denaturation during the sterilization process, thus impairing osteogenesis. Moreover comminuted fractures are known to heal less well because close approximation of the bone fragment is often difficult. There are recent reports that large bone flaps have a higher resorption rate.1016) Piedra et al.19) found that freezer times greater than 6 weeks led to a 3-fold increase in BFR (42% vs. 14%). Also, younger age has been identified as a risk factor for BFR by some authors.81621)
The high infection and BFR rates following cranioplasty raise important questions regarding the optimal sterilization and preservation methods. However, there are currently no standardized guidelines for sterilization and preservation of skull bone flaps for cranioplasty. Im et al.13) compared two sterilization methods, and found no significant difference in bone resorption rates between ethylene oxide gas sterilization and chemical sterilization. Several authors have investigated methods for preserving bone flaps for cranioplasty. These methods can be divided into two categories; those that retain the bone flap in the patient's body and those that store the flap extracorporeally.13141822) For extracorporeal preservation, cryopreservation has become the most widely used technique. However, complication rates appear to vary with the freezing temperatures, and we ourselves maintained flaps in room air in our series. Hence, further clinical studies will be needed to establish the best method of bone flap preservation.
Our study has several limitations. First, the number of complications was too small to identify significant risk factors. Nevertheless analyzing the risk factors for BFR is important because it can help to judge the prognosis of patients who are planned to undergo cranioplasty. Therefore further clinical studies with a much larger affected population are needed. Also ours was a retrospective study from a single institution, not a prospective trial, and there was no control group to establish the relationship between bone flap preservation and BFR.
Go to :
Conclusion
DC has become an inherent part of the treatment of life-threatening ICP, but many questions regarding cranioplasty remain unanswered. We have shown that cerebral infarction and TBI are possible risk factors for BFR after cranioplasty. To more definitively elucidate which factors affect BFR, a prospective controlled study with a large number of patients is needed.
Go to :
 XML Download
XML Download