

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The vertebral fractures is the most common complications of osteoporosis.13) These fractures result in significant mortality and morbidity including prolonged and intractable pain.4,13) Percutaneous vertebroplasty, a therapeutic procedure for filling the collapsed vertebral body with polymethylmethacrylate, provides pain relief.2,4) In general, percutaneous vertebroplasty is simple and safe if performed under continuing fluoroscopic control and technical precautions. Vertebroplasty has the potential risk of serious complications such as leakages of bone cement, cardiopulmonary complications, infection and the new fractures of the adjacent vertebrae.6,7) We present a case of extraspinal leakage after vertebroplasty at our hospital.
Go to : 
Case Report
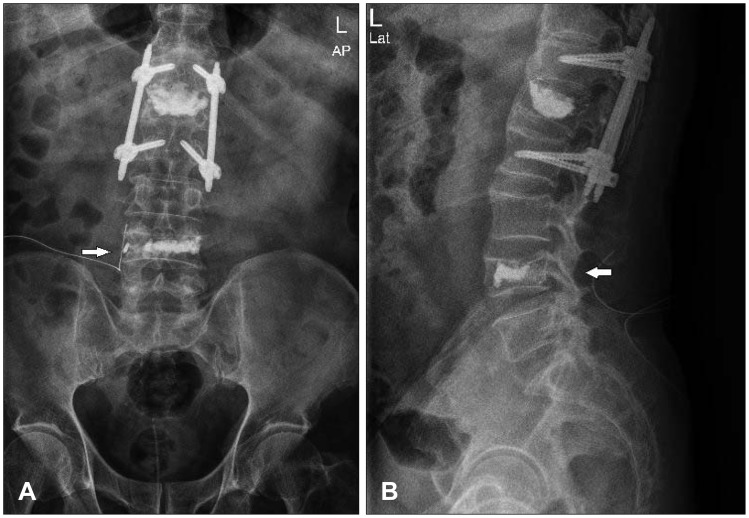
A 73-year-old male was admitted to our hospital for low back pain after slip down at one day earlier. After radiologic evaluation, acute osteoporotic compression fracture of the L4 vertebra was found. The patient had experienced L1 vertebroplasty and T12-L2 screw fixation for L1 compression fracture at another hospital before 2 years ago. Percutaneous vertebroplasty for L4 vertebra was performed under fluoroscopic guide. After incision of the skin, an 11-guage vertebroplasty needle was placed percutaneously on the posterior part of the vertebral body via bilateral transpedicular approach. The needle was pushed through the cortex, situated the center of the pedicle as possible, and then directed into the vertebral body. The anterior third of the body was an ideal location for the needle placement. The contrast medium (Iohexol) was injected to estimate bone cement distribution and minimize bone cement leakage and intraoperative complication such as pulmonary thromboembolism. When a thin toothpaste consistency was achieved, the bone cement was injected into the vertebral body under continuous fluoroscopic control. The filling process was stopped immediately when leakage of bone cement was observed into lateral space of body. After the procedure, his back pain was improved immediately. But he complained severe pain which radiates down the right leg on standing position. The patient was unable to bear weight on his right leg after the procedure. Neurologic examination revealed right leg hypoesthesia but straight leg raising test was negative. Lumbar simple X-rays after procedure showed leakage of bone cement to right lateral side of the L4 vertebral body (Figure 1). Lumbar computed tomography (CT) scanning revealed extraforaminal leakage of bone cement to outside of right L4 pedicle and it caused significant compression of L4 nerve root (Figure 2). The leaked bone cement along the L4 nerve root was removed carefully via paraspinal muscle-splitting approach. During surgery, two pieces of bone cements were removed carefully. Two whitish bone cements were located in the right lateral space of L4-5 body and the intervertebral foramen (Figure 3). After operation, severe right leg radiating pain and hypoesthesia were much improved. Postoperative lumbar spine plain images show that the leaked bone cement along right L4 nerve root was disappeared (Figure 4). After operation, severe right leg radiating pain and hypoesthesia were much improved. The patient was discharged on the tenth postoperative day.
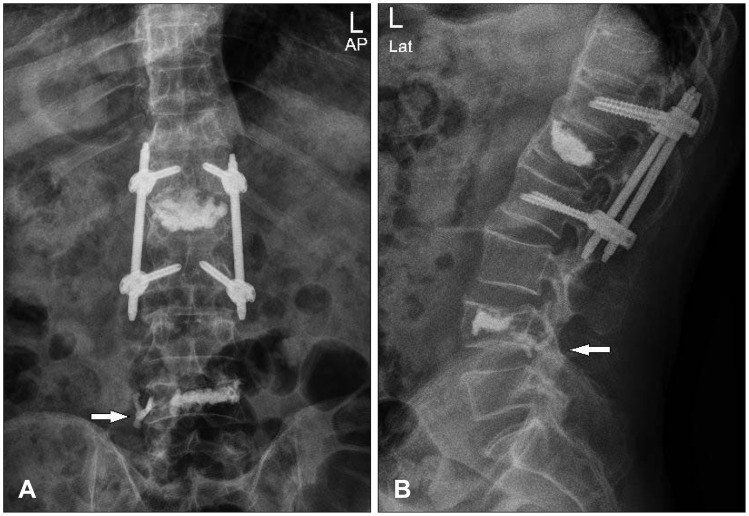 | FIGURE 1Lumbar spine plain images were taken after L4 vertebroplasty. Anterior-posterior (AP) view (A) and lateral view (B) show that cement leakage spread along the posteroinferolateral margin of L4 vertebra (arrow).
|


Go to :
Discussion
Complications related with vertebroplasty are not uncommon such as cement extravasation, pulmonary embolism, infection, epidural hematoma, systemic toxicity, and vertebral body fractures.1,7,8) Among the commonest complications, cement extravasation has been estimated in 70% cases for vertebroplasty procedures.3,5) Most of the cement extravasation is asymptomatic but, disastrous complications causing paraparesis have been also reported in the literature.5,7,12)
The biplanar fluoroscopy is the best way to monitor the leakage of cement in procedure of vertebroplasty, but sometimes it is difficult to judge the leakage of cement after injection of the contrast medium. Therefore, CT should be recommended if any kind of leakage was suspected. Yeom et al.14) described three different types of leakages of cement after vertebroplasty such as type B (via basivertebral vein), type S (via segmental vein), and type C (via cortical defect). Nieuwenhuijse et al.9) recommended that the high viscosity of bone cement should decrease the rate of cement leakage during vertebroplasty. Due to high risk of pedicle fracture during vertebroplasty, cement leakage via pedicle violation can cause significant morbidity.11)
Park and Kim10) mentioned technical tips while taking entry into the pedicle and the vertebral body. The bone access needle can be advanced through the center of pedicle with use of a tunnel vision technique (turn the C-arm obliquely until pedicle can be visualized at its widest and roundest) and verification of needle trajectory at midpedicular level and posterior surface of vertebral body on lateral view. On anterior-posterior view, if the tip is located too medially, the medial cortical wall of pedicle may be damage and leading to spinal canal violation. If the tip is located too far laterally, lateral cortical bone damage and lateral violation could occurred.
In our case, the reason of cement leakage might be presumed. The tip of needle located more laterally when needle tip is located in the pedicle and vertebral body. So pedicle and lateral end plate damages ware occurred.
Go to :
Conclusion
We experienced a case of lumbar nerve root compression by leaked bone cement after vertebroplasty. Proper entry point of trocar, keeping trocar within pedicle and proper position of trocar between the pedicle and spinous process under biplanar fluoroscopy view would be help to prevent leakage of bone cement after vertebroplasty.
Go to :
 XML Download
XML Download