

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Pediatric head injury is a major cause of death in children. Children have a relatively larger head in relation to their torso, which makes them more vulnerable to head injuries. Stratifying head injuries according to risk factors is very important to improve the prognosis of the injuries, especially when the risk relates to surgical mortality. However, it is hard to find reports on the preoperative estimation of the risk of surgery of head injuries.5) One of the specific features of young children is that the skull is malleable, and its sutures are tightly adhering to the underlying dura and venous sinus. These characteristics, in association with the small amount of total blood volume, can result in a specific fatal type of skull fracture, which is unique to infancy.
Here, we report a case of such a fatal type of head injury related to the specific anatomical characteristics of infants. A fracture crossing the midline, with wide fracture line, resulted in a serious injury accompanied by tearing of the underlying adhering sagittal sinus. Because of the small amount of total blood volume in this age group, there was no sufficient time for the adequate management of the sinus injury and the patient died due to severe edema related to the hypovolemia and sinus injury.
Case Report
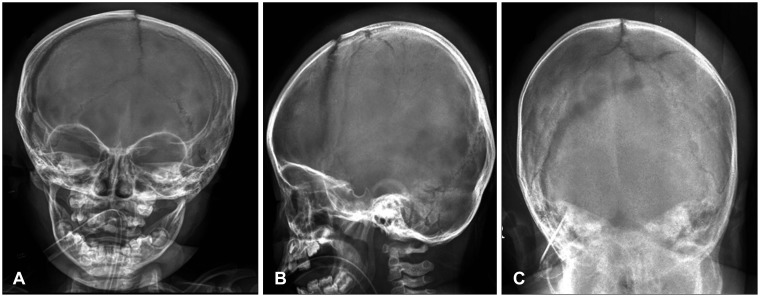
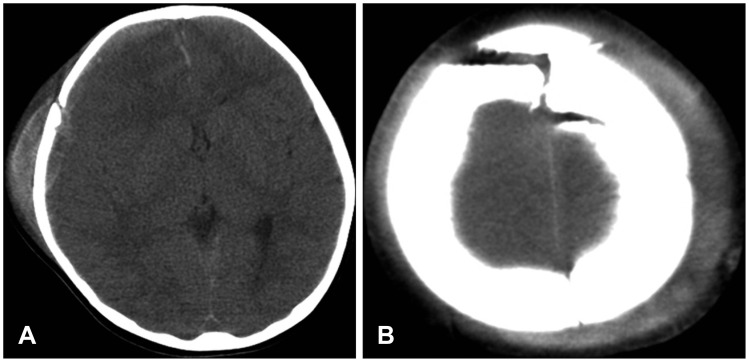
A 23-month-old female patient presented with semicomatose state after falling from a second floor height, following which generalized tonic and clonic seizures occurred. The patient's pupils were fully dilated and fixed to light bilaterally. Plain skull films showed a diastatic fracture of the right coronal and sagittal sutures and the fracture extended into the left parietal bone. The sutures were separated by a small gap between the bones (Figure 1). An emergency computed tomography (CT) scan showed a moderate amount of subdural hematoma along the right convexity and midline shifting (Figure 2).
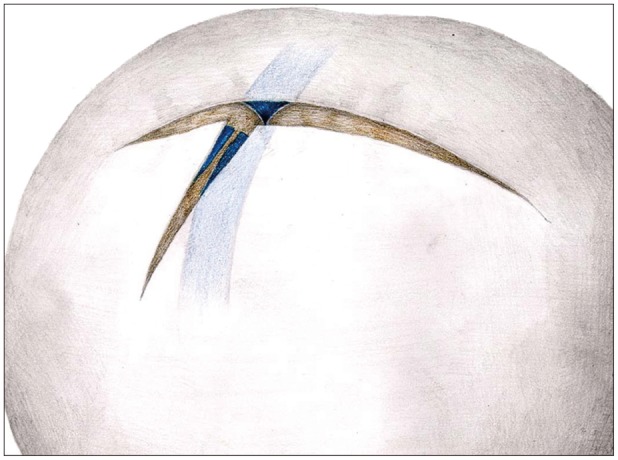
An emergency craniectomy and hematoma removal were performed. After scalp incision, a profound amount of bleeding emerged from the fracture site. The craniectomy and dural opening showed that the hemorrhage was coming from the separated sagittal sinus underlying the fracture (Figure 3). The blood loss was massive and hypovolemic shock developed soon after scalp incision, which was corrected with transfusion. The patient died 2 days after the operation due to severe brain edema possibly related with sinus obstruction and hypovolemic shock during the operation.
Discussion
Young children, especially those below 2 years of age, have specific anatomical and physiological features of the head.1) These features explain why skull fractures without significant neurological deficits are relatively common after a head injury in this age group.4,5) Mann et al.5) demonstrated that patients below the age of 2 years have the highest incidence of fractures and the lowest incidence of intracranial hematomas because of their open sutures and the adherence of the dura to the inner table of the skull. Similarly, Herrera et al.2) reported that the presence of skull fractures in infancy was not correlated to the severity of the craniocerebral trauma. Our case shows that skull fracture like in our case can damage the underlying dura and venous sinus because of the tight adherence of the sagittal sinus to the overlying skull. Even though the age of our patient was 23-month-old, which is above the age of the definition of the infant, we used the terminology interchangeably in this age bracket because the characteristics of the injury was unique in relation to an infant in terms of mechanism and clinical feature. In addition, special care should be paid to this patient in this age group. Kodikara and Pollanen3) reported a horizontally-oriented, widely-displaced fracture coursing over the vertex of the head due to a television toppling. Symmetrical bilateral skull fractures, as in their case, resulted from bilateral compression of the head between two surfaces. However, they did not mention the condition of the venous sinus. Our case had a bilateral skull fracture involving the diastasis of the sagittal suture. We postulate that the high-energy impact on the vertex, displacing the local area, resulted in the separation of the sagittal and coronal sutures and that overstretching of the underlying dura made a tear in the dura, which then involved the dural venous sinus.
Skull radiographs or CT scans are useful tools for investigating and predicting this kind of devastating skull fracture. By this case we recommend that if surgery for hematoma removal must be performed, the tearing of the dural venous sinus and massive bleeding should be anticipated, and great care should be taken to prevent and manage the profuse bleeding and early hypovolemic shock that may occur.
 XML Download
XML Download