

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Chronic subdural hematoma (CSDH) is one of the most common disorders in the field of neurosurgery.2) The current understanding of the mechanism of development of CSDH is that damage to the bridging veins by minor head trauma results in a collection of hematomas in the subdural space.15) Then, the hematomas form a vessel-rich outer membrane.18,21) Fragility of this neovasculature leads to repeated microbleeding and increases the permeability of the membrane, resulting in the development of CSDH.2,3,13,14) The known risk factors of CSDH are trauma, old age, brain atrophy, alcohol abuse, seizure, coagulopathy, the use of anti-platelets, and the use of anticoagulants.7,10) In this study, we focused on the fact that some patients do not develop CSDH after head trauma and proceed through therapy without any complications, while others need additional surgeries to treat CSDH. Assuming there are differences between the patients who develop CSDH and those who do not, we investigated the various known risk factors, along with the computed tomographic findings at the time of the head injury.
Go to : 
Materials and Methods
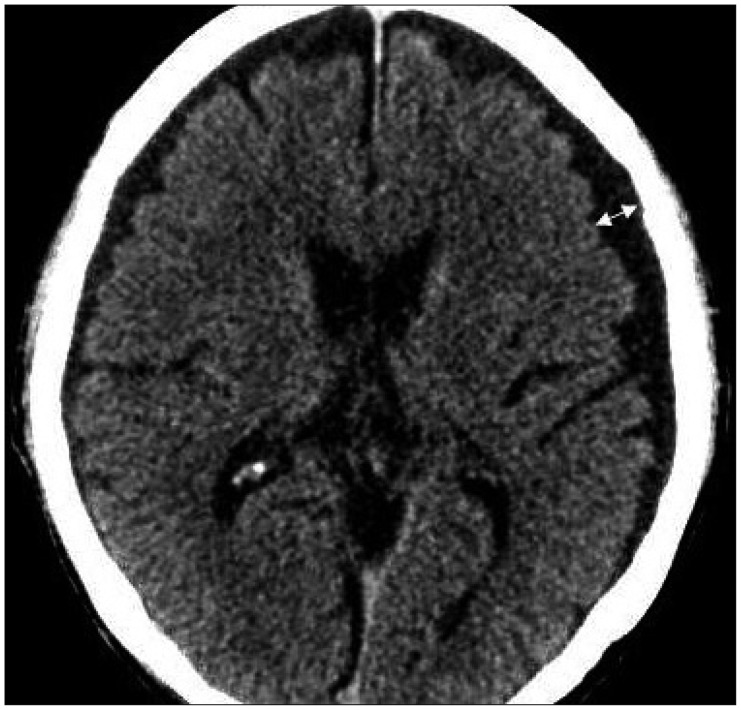
We conducted a survey of 277 patients who scored over 13 on the Glasgow coma scale who received treatment at our institution after minor head trauma in the period from January 2012 to December 2013. Patients were enrolled prospectively and their medical records were reviewed retrospectively. All the patients did not require surgery at the time of their arrival. During the follow-up period, the 20 patients who required surgery to treat CSDH were designated as the patient group, while the remaining 257 patients who did not develop CSDH after minor head trauma and completed treatment were selected as the control group. Head trauma, out of many other factors, was set as the controlled variable. Age, gender, and the history of diabetes mellitus (DM), hypertension, cerebral infarction, cardiac disease, hematologic disease, and epilepsy were investigated as the factors contributing to progression of CSDH after minor trauma. The medication history of antiplatelet and anticoagulant agents was also surveyed, as well as the smoking and drinking habits of subjects. The presence of acute subdural hematoma (ASDH) in the convexity, accompanying hemorrhage and encephalomalacia, and the maximum distance from skull to cerebral parenchyma (Figure 1) were investigated by examining the patients' initial computerized tomography (CT) scans. In our study, cardiac disease included valve disease, arrhythmia, and ischemic heart disease. The diseases that could cause coagulopathy, such as hematological malignancies, were defined as hematologic disease. In cases where the patients' initial brain CT scans showed cerebral contusion, subarachnoid hemorrhage, epidural hemorrhage, or intracerebral hemorrhage, we defined the finding as an accompanying hemorrhage. The statistical analysis was performed using Window SPSS version 20.0 (SPSS Inc., Chicago, IL, USA). Statistical analyses included chi-square test, Fisher's exact test and multivariate logistic regression analysis to assess the relationship between CSDH and various factors. Differences were considered statistically significant if the p value was less than 0.05.
Go to :
Results
Demographic data, medical history, social history, and CT findings are summarized in Table 1.
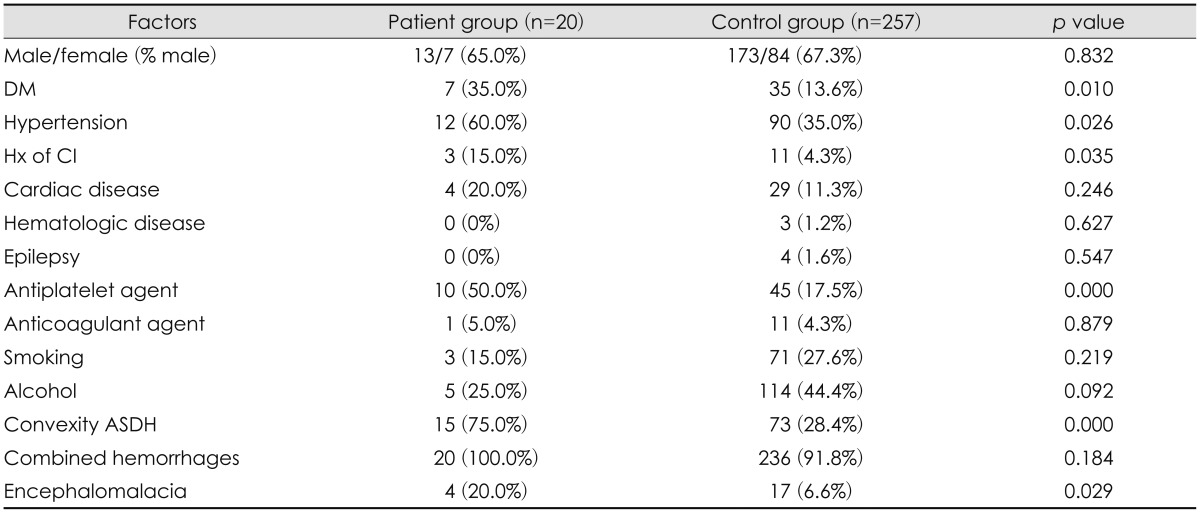
The number of patients enrolled in the study was 277, with an age range of 0 to 94 years, and a mean age of 53.9 years. The average age of the patient group was 67.5 years, while that of the control group was 52.9 years, showing that the patient group was statistically significantly older than the control group (p=0.014)(Figure 2). Thirteen male patients (65%) and 7 female patients (35%) were in the patient group, while 173 male patients (67.3%) and 84 female patients (37.7%) made up the control group with males contributing a little higher number in both groups, without a noticeable significance in the gender difference (p=0.832).
In the patient group, there were 7 (35%) patients with DM and 12 (65%) patients with hypertension, while there were 35 (13.6%) patients with DM and 90 (35.0%) patients with hypertension in the control group. The presence of DM or hypertension showed a statistical significance between groups (p=0.010, p=0.026).
The numbers of the patients with a history of cerebral infarction were 3 (15%) in the patient group and 11 (4.3%) in the control group, which was also statistically significant (p=0.035).
With regards to medication history, the administration of antiplatelet agents presented a statistically significant difference between the two groups (p=0.000); 10 in the patient group (50%), 45 in the control group (17.5%).
The brain CT scans taken on the time of admission were examined. A higher percentage of subjects in the patient group (15 patients, 75%) had ASDH in the convexity from the trauma than that of patients in the control group (78 patients, 28.4%) at a level of statistical significance (p=0.000).
Four subjects in the patient group (20%) had encephalomalacia, while 17 patients (6.6%) in the control group had the affliction with statistically significant (p=0.029).
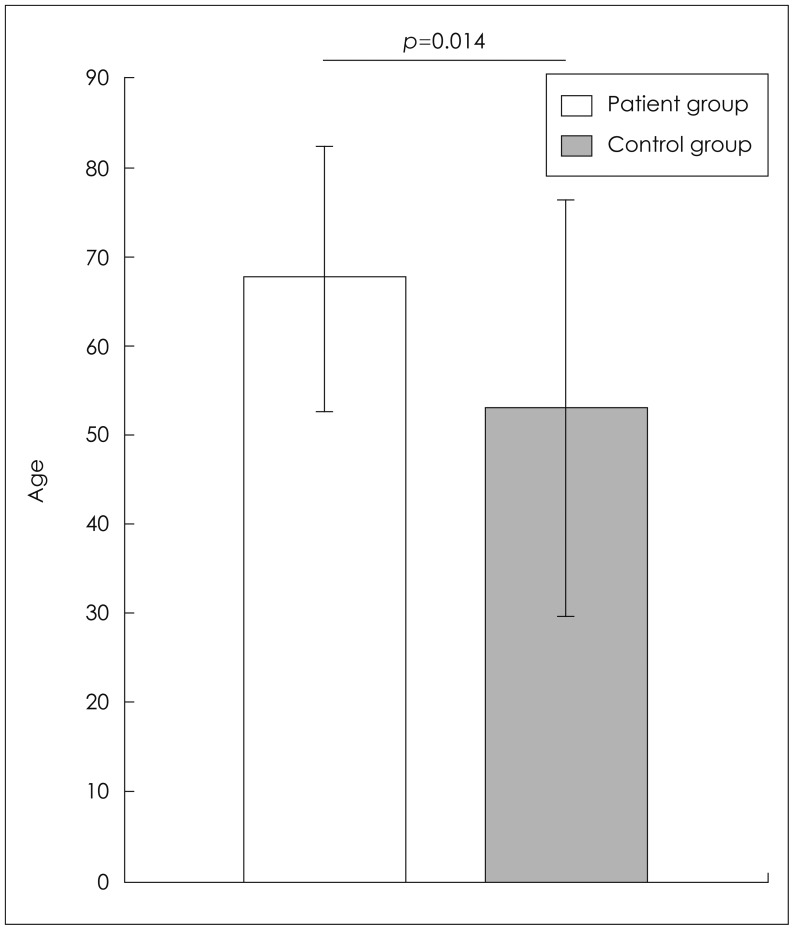
The brain CT scans taken right after the trauma were used to measure the maximum distance between the skull and the cerebral parenchyma. The average maximum distance of the patient group (7.15 mm) was much longer than that of the control group (1.35 mm) and the difference was statistically significant (p=0.000)(Figure 3). The receiver operating characteristic curve was drawn by plotting the occurrence of CSDH according to the maximum distance between the skull and the brain parenchyma. It was determined to be reliable test model due to its large area under the curve. We found that the distance between the skull and parenchyma as 3.52 mm can be a cutoff value, yielding 90.0% sensitivity and 90.7% specificity (Figure 4).
 | FIGURE 3Bar graph shows the average maximal distance between skull and brain parenchyma of the two groups. The patient group had a statistically significant longer distance than control group (p=0.000).
|
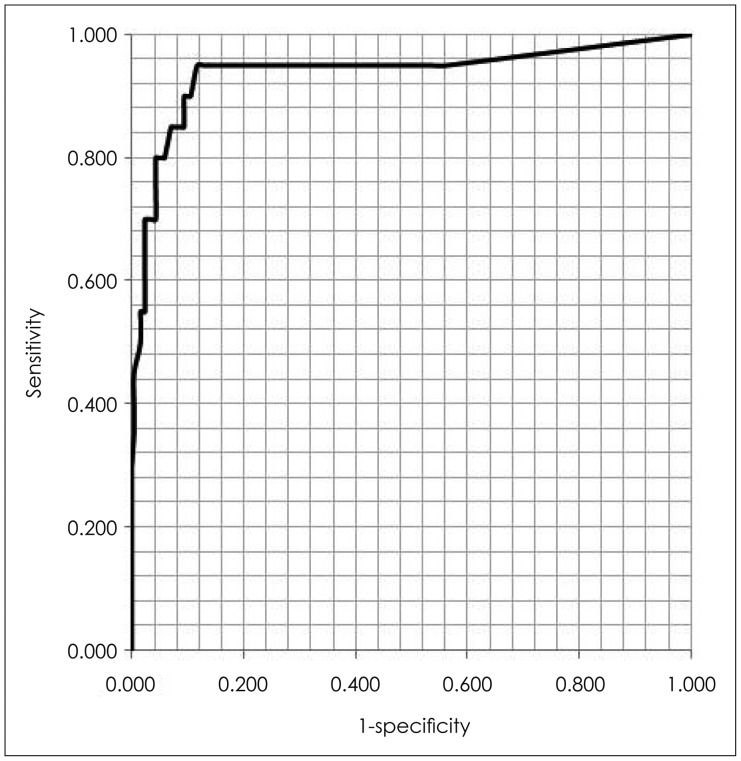 | FIGURE 4Receiver operating characteristic (ROC) curve of the maximal distance between the skull and brain parenchyme. In a ROC curve, the true positive rate (sensitivity) is plotted against the false positive rate (1-specificity) for different cut-off points of a parameter. In this graph, 3.52 mm is the cutoff value of 90.0% sensitivity and 90.7% specificity. The area under the ROC curve is a measurement of how well a parameter can distinguish between two groups. Here, the maximal depth between the skull and brain parenchyma is a good parameter for distinguishing between the two groups.
|
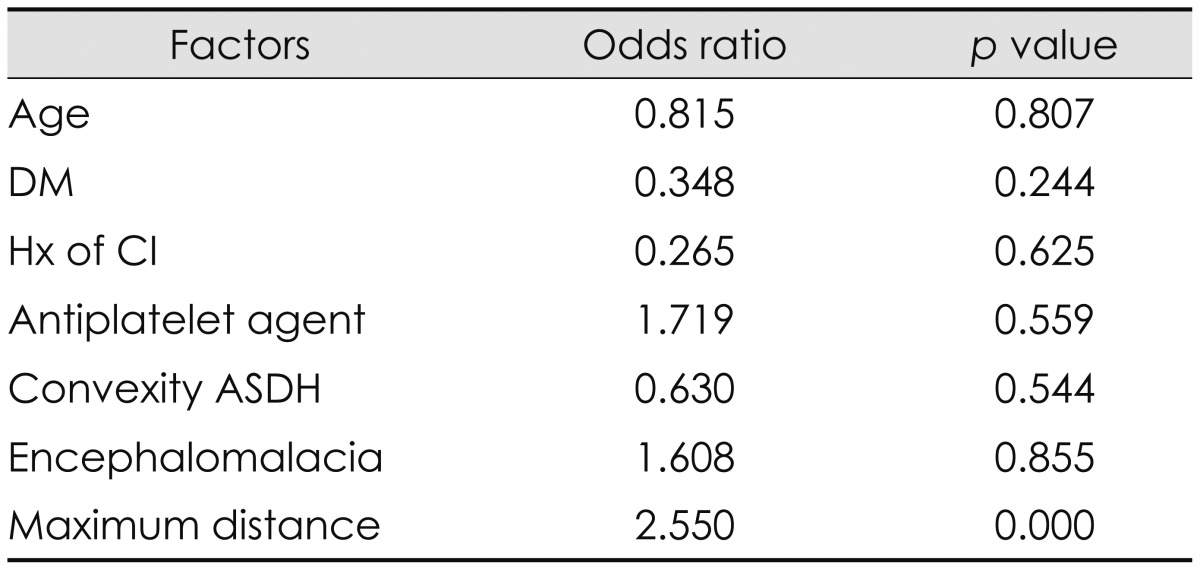
The multivariate logistic regression analysis was used to verify the correlation between the statistically significant factors and CSDH occurrence. As a result, only the maximum distance between the skull and the cerebral parenchyma showed a reliable correlation with CSDH occurrence (p=0.000), while the other factors failed to show any remarkable statistical significance (Table 2).
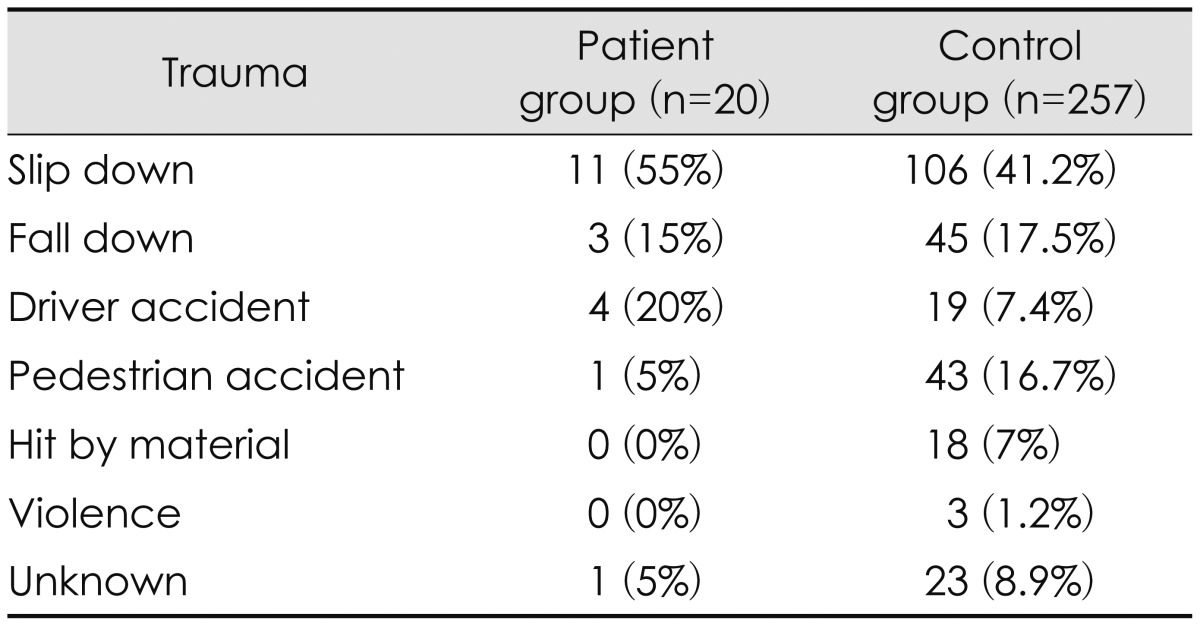
Each group was classified according to the type of trauma. Slipping down stood out as the most common cause of trauma but with no statistical significance between the two groups (p=0.236)(Table 3).
Go to :
Discussion
Unlike other studies,7,10) this study demonstrates that the presence of DM or hypertension significantly influences the occurrence of CSDH after minor head trauma. On the contrary, a study conducted by Yamamoto et al.22) reported that the hyperglycemia in DM patients leads to the hyperviscosity of blood and increases the intravascular osmotic pressure, resulting in a reduced probability of CSDH recur. However, considering the fact that one of the major complications of DM is capillary vasculopathy such as retinal hemorrhage, and the fact that micro-bleedings and the exudation of immature capillaries surrounding the CSDH outer membrane are the major mechanisms in developing CSDH, the capillary vasculopathy in DM patients affects the immature capillaries around the outer membrane of the subdural hematoma after head trauma, and consequently results in the development CSDH.20)
Also, in the case of patients with hypertension, higher blood pressures put more pressure on the immature capillaries around the outer membrane have to endure, increasing the probability of repeated capillary injuries and micro-bleedings. Even though there are few preexisting studies on the impact of hypertension on the CSDH,8) additional studies need to be performed to confirm a correlation between hypertension and CSDH.
It is known that the old age is associated with CSDH, as there is a higher CSDH prevalence rate among the elderly.1,5,6) The fragility of the bridging veins and accompanying cerebral atrophy from the aging process are considered as the major factors causing the increased prevalence.5,19) As aging progresses, the volume of the cerebral parenchyma shrinks, resulting in an increase of the subdural space between the skull and the cerebral parenchyma. The enlarged subdural space enables the brain to move around the skull while patient ambulates, and the vulnerable bridging veins can be injured easily with a minor head trauma.9,12,23) The correlation between the occurrence of CSDH and old age was also confirmed in this study, and there was a tendency to develop post-traumatic CSDH among the patients with larger subdural spaces due to cerebral atrophy. The reason why the history of cerebral infarction and the presence of encephalomalacia are correlated with CSDH occurrence in this study can be explained by considering the same mechanism described above. The presence of encephalomalacia after the brain injury, such as cerebral infarction, results in the reduction of brain parenchyma volume, which enlarges the subdural space between the skull and brain parenchyma, and consequently results in higher tendency of post-traumatic CSDH.16)
A study from Lindvall and Koskinen,10) which analyzed 71 patients with CSDH concluded that the administration of antiplatelet or anticoagulation agents contributed a significant difference in CSDH occurrence in the patients without trauma compared to the patients with trauma. Another study conducted by Reymond et al.17) analyzing 198 patients with severe head trauma also reported that there was a statistical significance between the administration of antiplatelet or anticoagulation agents in CSDH occurrence. Considering the analogous result in the preceding two studies, the same outcome was expected when analyzing our data. However, there was no statistically significant difference between using anticoagulation agents and the occurrence of CSDH, while there was a significant correlation between the use of antiplatelet agents and the occurrence of CSDH. While the preceding studies analyzed patients who already developed CSDH or had severe head trauma, we included all the patients with minor head trauma, which may explain the difference in the outcome. Also, the fact that the patient group only had a limited number of the patients may be related to the difference as well.
It was expected that there would be a correlation between CSDH occurrence and the patients with cerebral infarction or with cardiac disease, as they are commonly administered antiplatelet or anticoagulant agents.10) The actual study showed a higher ratio of patients with cerebral infarction or cardiac disease in the patient group than in the control group. However, only the history of cerebral infarction demonstrated a statistically significant difference, while the presence of cardiac disease failed to show a statistical significance. With regard to cerebral infarction, aside from using antiplatelet agents or anticoagulants, other co-factors, such as a decrease in brain volume due to encephalomalacia after infarction, could influence the outcome. Also, the insufficient number of the patients analyzed in the patient group is likely the reason why we could not find a significance relationship between CSDH occurrence and the presence of cardiac disease.
Generally, the hematologic diseases that cause coagulopathy are known to be risk factors for post-traumatic CSDH occurrence.1,4) The history of epilepsy is also expected to be a risk factor of CSDH since it can cause repeated seizures.1,11) We began our analysis considering these known concepts, but the history of hematologic diseases and epilepsy showed no significant differences in our study. Yet, there was no patient with a history of hematologic diseases or epilepsy in the patient group, and a very small number of the patients with a history of hematologic diseases (1.1%) or epilepsy (1.4%) were present among the entire test population. It is assumed that the limited number of patients analyzed in the study impacted the result as well.
Limitations of the current study include the small number of patient group and the retrospective nature of the study design. However this study creatively demonstrated the predictive factors of CSDH in patients with minor head trauma.
Go to :
Conclusion
Based on the results of this study, the predictive factors of post-traumatic CSDH occurrence are old age, preexisting DM, hypertension, and history of cerebral infarction, the presence of ASDH in the convexity found in brain CT scans taken right after the trauma, encephalomalacia, and an enlarged subdural space between skull and brain parenchyma. When treating patients with minor head trauma accompanied by those risk factors, physicians must pay careful attention to the possibility of post-traumatic CSDH and need to continuously observe the patients.
Go to :
 XML Download
XML Download