

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Tetralogy of Fallot (TOF) is the most common cyanotic congenital heart disease [1], with only a few patients reaching adulthood without surgical correction; ten percent may survive to their 30s but only 3% reach their 40s or older [2] and survival beyond the seventh decade of life is even rarer [3].
TOF comprises obstruction to right ventricular outflow tract (RVOT; pulmonary stenosis [PS]), ventricular septal defect (VSD), overriding of the aorta, and right ventricular hypertrophy. Systemic hypoxemia correlates with the degree of RVOT obstruction. TOF with hypoxic spells present as periods of profound cyanosis that occur because of almost total RVOT obstruction.
The patients with severe RVOT obstruction have more frequent early hypoxic spell events. Unrepaired TOF patients with mild to moderate RVOT obstruction may be clinically silent until adulthood. So, hypoxic spell typically occurs in a crying infant but is rare in an adult [4].
We reported the case of a 75-year-old natural survivor with uncorrected TOF presenting with hypoxic spell. To our best knowledge, this is the oldest case of natural survivor with uncorrected TOF in Korea and the oldest patient presenting hypoxic spell worldwide.
Case
A 75-year-old male patient visited the emergency department of our hospital due to cyanosis and dyspnea. He recently had worsened dyspnea and heart function in class III, New York Heart Association (NYHA). His perinatal history was unknown. He had been diagnosed with TOF 20 years ago but no surgical correction was done due to nearly asymptomatic childhood. He occasionally complained of exertional dyspnea without hypoxic spell. Recently, he had become symptomatic, with progressive dyspnea and cyanosis. On visiting the emergency department for dyspnea, he had been experiencing aggravated hypoxic spell and chronic heart failure and was on medications for systemic hypertension and atrial fibrillation.
At presentation, he was alert but looked tired and lethargic. He had clubbing on the fingers and toes, central cyanosis, and pitting edema on both lower legs. The blood pressure was 158/94 mmHg. The heart rate was irregular at 97 beat per minute, and the respiratory rate was 24 breaths per minute with increased respiratory effort. The oxygen saturation was 90%–94% initially, but abruptly he showed tachypnea and lip cyanosis with decreased saturation to 60%–83% by pulse oximetry monitoring. Initially, he had an ejection systolic murmur in the pulmonary area and a diastolic regurgitant murmur on the left sternal border, but at the time, we found no audible murmur.
Due to hypoxic spell, we promptly initiated oxygen supply and recommended the knee-chest position. After oxygen supply (5 L/min via mask), oxygen saturation was improved to 90%. He frequently showed hypoxic spell without associated significant events. Electrocardiogram showed atrial fibrillation with a heart rate of 98 beats/min and incomplete right bundle branch block with QRS duration of 104 msec. The chest radiography showed severe cardiomegaly (cardiothoracic ratio 73.5%), pulmonary edema and pleural effusion. The pulmonary dilatation was observed (Fig. 1).
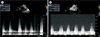
An echocardiography showed overriding of the aorta, anterior malalignment interventricular septum, VSD, mainly subvalvular PS with static and thickened pulmonary valve (PV), moderate pulmonary regurgitation, narrowing and hypertrophy of RVOT and post-stenotic dilated pulmonary artery (PA) with impaired right ventricular systolic function (RV tricuspid annular plane systolic excursion 13.5 mm). The right atrium was dilated and a moderate tricuspid regurgitation with slightly D-shape interventricular septum was present. The left atrium and left ventricle (LV) were slightly dilated but showed markedly impaired systolic function with ejection fraction of 23% (both M-Mode and Simpson method) (Fig. 2). During extremely resting state, the patient showed relatively mild stenosis of the RVOT (velocity, 3.62 m/sec), Bidirectional shunt but predominantly left-to-right through the VSD (pressure gradient [PG], 117.08 mmHg) (Fig. 3). But, during hypoxic spell, the echocardiography changed to predominantly right-to-left shunt through the VSD (PG, 80.49 mmHg) and more severe subvalvular PS (velocity, 5.54–6.14 m/sec) (Fig. 4).
Chest high resolution computed tomography (HRCT) showed no evidence of pulmonary thromboembolism, but revealed cardiomegaly and pericardial effusion with post-stenotic dilated pulmonary trunk. Interlobular septal thickening and patchy ground-glass attenuation were seen in both lungs, consistent with pulmonary edema.
Laboratory studies revealed hemoglobin level of 14.5 g/dL, hematocrit of 45%, platelet count of 138,000/µL, and NT-proBNP >35,000 pg/mL. Other cardiac enzymes were within normal limits. Arterial blood gas analysis showed pH 7.38; partial pressure of carbon dioxide (PCO2) 33 mmHg; partial pressure of oxygen (PO2) 53 mmHg; bicarbonate (HCO3-) 19.5 mmol/L; and oxygen saturation 86% under oxygen supply.
The patient has already received treatment with angiotensin-converting-enzyme inhibitor (perindopril) for systemic hypertension and amiodarone for atrial fibrillation. We newly added furosemide, spironolactone, digoxin and low molecular weight heparin (LMWH) for prevention of pulmonary thromboembolism. Sodium bicarbonate was administrated for correction of metabolic acidosis. We kept the patient in knee-chest position under non-rebreathing mask with 100% oxygen. The patient gradually showed improvement of general symptoms. However, hypoxic spell persisted despite knee-chest position, oxygen supplement, normal saline intravenous infusion, morphine and oral beta blocker.
On the 4th hospital day, bosentan (endothelin receptor antagonist) was added and LMWH was substituted with clopidogrel. Subsequently, he presented no more hypoxic spell and attained oxygen saturation of 90%–93% with oxygen supply. His general condition and oral intake were noticeably improved on the 5th hospital day and his oxygen saturation was maintained between 88%–93% without oxygen. He was considered well enough to be discharged on the 7th day and went to sanatorium for further recuperation. The oral medications after discharge included bosentan, furosemide, spironolactone, clopidogrel, amiodarone, and perindopril.
After discharge, he was doing well without dyspnea and oxygen saturation was maintained above 90% without oxygen supply. He and his family refused any surgical treatment and any invasive procedure mainly due to concerns of his old age and comorbidities.
Discussion
The hypoxic spell is an episodic central cyanosis due to total occlusion of right ventricular outflow in a patient with a congenital heart disease, such as TOF. It is characterized by paroxysm of hyperpnea, irritability and prolonged crying, increased cyanosis and decreased intensity of heart murmur. If not treated in time, it may lead to limpness, seizure, neurological deficit and death [5]. It is most likely to be seen in a child less than 2 years old, upon waking up in the morning and following crying events [6], but is rare in adult. Anders and Fuchshuber [4] reported cyanotic spell in a 69-year-old woman with pentalogy of Fallot, who was younger than our patient. Our patient showed relatively moderate stenosis of the RVOT, with a bidirectional shunt predominantly left-to-right through the VSD at rest, explaining the absence of severe cyanosis in his childhood.
In TOF, the level of cyanosis and onset of cyanotic spell is determined by the systemic vascular resistance (SVR) and degree of RVOT obstruction. Some theories have been proposed as possible explanation for the cause of hypoxic spells [5]. Guntheroth et al. [7] reported that episodes of paroxysmal hyperpnea are the cause rather than the effect of cyanotic spells. The hypoxic spell of our patients was initiated by hyperpnea and the cause of worsening hyperpnea was not corrected. Nevertheless, his anxiety may have influenced increasing hyperpnea.
Typically, hypoxic spells occur early in the morning. The possible aggravating factors are anxiety, fever, anemia and sepsis. But, our patient's hypoxic spell was not related to other causes such as specific time, feeding, and bowel movement except anxiety.
Variable factors could have affected the patient's hemodynamics and contributed to prolonged survival; however, the hemodynamic balance is not clearly explained. The PA pressure measurement through cardiac catheterization is necessary to know more accurate hemodynamics. However, the patient was so old and the caregivers did not want to do any further studies.
We think that the limit of this study is not measuring the data more accurately. Although TOF and consequent PA hypertension (PAH) are difficult to compatible at all, but when combined with computed tomography and echocardiography findings, if the infundibular stenosis secondary to Eisenmenger syndrome occurs, the PA pressure would be very high, so there would not be high PG at infundibulum. But, the patient had a lot of PG at infundibulum. In addition, PA is less than aorta and there was no central-peripheral PA discrepancy. The patient was considered to be more appropriate for TOF. The PV of the patient was very static and thickened. The subvalvar PS was main, but there was also mild valvar PS. When PG was measured by echocardiography, mild valvar PS was also present. Therefore, there was no problem in diagnosing TOF in this patient.
If echocardiographic data were available for the patient in the youth, it would be more meaningful to observe the changes in the mild TOF over time. Unfortunately, we could not get it because it was too old data.
Prolonged survival of patients with uncorrected TOF is often associated with a well-developed LV [8]. PAH might be caused by pulmonary agenesis, hypoplasia and/or thrombosis, inadequate closure of the VSD, relief of the PS, or an excessively large prior systemic-to-pulmonary shunt. Moreover, patients with TOF who are diagnosed as inoperable because of the presence of PAH show similar hemodynamic and clinical features to patients with Eisenmenger syndrome [9]. In our patient, the LV function was not good but systemic hypertension may also play a role in the balancing of pressure between the two ventricles.
The hemodynamic consequences for both the right and left ventricles are significant. In infancy, pulmonary vasodilator is not used for hypoxic spell, because decreasing pulmonary vascular resistance may increase left to right shunt. Our patient had no possibility of total correction, hence we considered more symptomatic than curative treatment.
Pulmonary vasodilator is not a treatment option for hypoxic spell but since the symptom showed no improvement to typical hypoxic spell treatment, we tried bosentan for pulmonary vasodilation. In cases without systemic hypertension, medication for increasing SVR like intravenous phenylephrine is indicated. In our patient, the hypoxic spell markedly improved after administration of bosentan; however, drug action mechanism is not exactly known.
Finally, considering the benign course of this congenital heart disease, we performed conservative medical treatment alone without invasive diagnostic or therapeutic management.
Currently, adult patients with uncorrected TOF are a rarity. Nevertheless it is important to improve their quality of life and relieve symptoms such as hypoxic spells. This case report highlights the need for additional study on treatments to improve the hypoxic spells for adulthood.



 XML Download
XML Download