

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
A new humanized monoclonal antibody against the interleukin-6 receptor (IL-6R), tocilizumab (Actemra®) is currently used for the treatment of rheumatoid arthritis (RA) patients who show inadequate responses to conventional disease modifying anti-rheumatic drugs or tumor necrotizing factor (TNF)-α blockades [12]. However, despite comparable therapeutic efficacy, tocilizumab was reported to exert several unwanted effects including dyslipidemia, upper respiratory tract infections, nasopharyngitis, headache, and high blood pressure [345]. In addition, some patients (less than 5%) experience tocilizumab-related transaminitis, although a significant increase in the levels of liver enzymes, over 5 times as high as normal reference ranges, is rare [345]. To our best knowledge, there have been no reports on significant liver toxicity with tocilizumab in Korean patients with RA to date. Hence, we report the case of 76-year-old woman with seropositive RA who showed tocilizumab-related liver toxicity.
Case
On July 23, 2014, a 76-year-old woman was admitted for fever and general weakness to Severance Hospital, Yonsei Medical Center (Seoul, Korea). She had been diagnosed with seropositive RA (rheumatoid factor 70 IU/mL, anti-cyclic citrullinated peptide antibody negative) one year ago and had received 2 mg of tacrolimus and 10 mg of prednisolone over the last 1 year. On October 2013, she had undergone lung segmentectomy (left lower lobe) for adenocarcinoma (stage 1). Sulfasalazine and non-steroidal anti-inflammatory drugs had been tried, but they were discontinued due to drug eruption and gastric ulcer bleeding, respectively. Also, methotrexate and leflunomide were not considered due to her reduced lung capacity and minimally developed interstitial lung disease. At that time, RA activity was well controlled.
On admission, her blood pressure was reduced to 82/54 mmHg, pulse rate was 144/min, respiratory rate was 24/min, and body temperature was 38.9℃. White blood cell (WBC) count was 13,710/mm3 (neutrophil 89%), C-reactive protein (CRP) level was 441.0 mg/L (reference, <8.0 mg/L), and erythrocyte sedimentation rate (ESR) was 102 mm/hr. The prothrombin time and activated partial thromboplastin time were within normal limits and fibrinogen was 4.68 g/L (reference, 1.6 to 4.5 g/L). Urinary analysis showed WBC 2+ and nitrite 1+, and urine culture study revealed the growth of Escherichia coli. She was clinically suspicious of septic shock due to urinary tract infection. She discontinued tacrolimus and begun to receive antibiotics. The dose of prednisolone was increased to 30 mg/day, considering septic condition and relative adrenal insufficiency, and it was tapered to 20 mg/day in 14 days. The infection-related symptoms and laboratory results were improved: WBC 7,170/µL, CRP level 56.2 mg/L, and ESR 28 mm/hr. Urine culture study showed no growth of bacteria. Aspartate aminotransferase (AST) and alanine aminotransferase (ALT) levels were 32 IU/L and 19 IU/L, respectively.
On August 14, 2014, she complained of pain in multiple joints including the bilateral wrist, hand, and foot joints, in which increased uptake was shown on whole body bone scan (Fig. 1). On physical examination, swelling and tenderness were present in all involved joints. CRP level and ESR increased to 82.5 mg/L and 75 mm/hr, and the 28-joint disease activity score (DAS28) was calculated at 6.3. We also considered the possibility of adult onset Still's disease (AOSD) because of a high level of ferritin (6,370 ng/mL); however, the patient did not present any other symptoms or signs, such as fever, sore throat, skin rash, or cervical lymphadenopathy, other than arthralgia. We concluded that RA had flared up rather than AOSD being present, and we carefully restarted 0.5 mg of tacrolimus. Thereafter, we gradually increased its dose to 2 mg, but the patient's symptoms were not much improved. The laboratory findings showed different patterns than those on admission: WBC and platelet counts were reduced to 3,960/µL and 80,000/µL, whereas AST, ferritin, and lactate dehydrogenase (LDH) levels rose to 103 IU/L, >15,000 ng/mL, and 548 IU/L, respectively. Fibrinogen level was 1.17 g/L, and we checked for soluble IL-2 receptor (sIL2Rα), which was 2,180 U/mL. Since she was suspected of reactive hyperplastic syndromes of histiocyte lineage, such as macrophage activation syndrome (MAS), she underwent bone marrow biopsy.
Histological examination of the bone marrow biopsy revealed a few individual areas of fat necrosis surrounded by macrophages showing cluster of differentiation 68 (CD68) positivity in immunohistochemical staining (Fig. 2), and frequent hemophagocytes were seen in bone marrow aspiration exam. She fulfilled the classification criteria for MAS by persistent fever, cytopenia affecting two lineages, low fibrinogen (<1.5 g/L), elevated ferritin (>500 ng/mL), increased serum sIL2Rα, and hemophagocytosis in bone marrow [6]. She received steroidpulse therapy (methylprednisolone 1,000 mg/day for 3 days), followed by 1 mg/kg/day of prednisolone. Tacrolimus was maintained, instead of the administration of etoposide, because the levels of ferritin and LDH slightly decreased and her platelet counts were nearly restored after steroid pulse therapy. AST also decreased to the normal reference range, and ferritin decreased to 11,810.9 ng/mL. MAS-related symptoms such as fever also improved.
Nevertheless, even though MAS was recovering, RA activity was not well controlled with DAS28 of 6.8. Thus, additional or substitutive therapy with tacrolimus was necessary for modulating RA activity. TNF-α blockade was contraindicated due to the patient's history of lung cancer. We started tocilizumab to treat RA. Considering the risk of infection and the patient's old age, we started it very carefully at a half dose, the dose of 4 mg/kg, biweekly. After 2 weeks from the first administration of tocilizumab, CRP level and ESR fell to 2.9 mg/L and 2 mm/hr, and furthermore, ferritin level was reduced to 9,120.6 ng/mL.
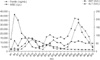
However, despite improved both clinical and laboratory findings, AST and ALT levels started to rise. As liver enzyme elevation was minimal at the first administration (less than 2 times the normal range), and symptom relief was remarkable, a second administration of tocilizumab was applied after 2 weeks from the former. Ten days after the second administration, AST and ALT levels rose to 207 IU/L and 181 IU/L, respectively, while ferritin levels continued to decrease to 2,138.9 ng/mL. Hepatitis viral serology test for hepatitis A virus, hepatitis B virus, hepatitis C virus, and Epstein-Barr virus were negative, and there were no laboratory results suggesting autoimmune hepatitis. Other drugs, such as antibiotics, that could injure the liver had been already discontinued after the first administration of tocilizumab. Furthermore, other laboratory and radiological results other than AST and ALT levels were relatively within normal reference ranges, different from the previous results at the time of the diagnosis of MAS. We concluded that tocilizumab might be the perpetrator of the liver toxicity rather than MAS activation, discontinued it, and restarted 0.5mg of tacrolimus with the maintenance of 10 mg of prednisolone. Aminotransferase fell to within normal ranges, and the disease activity of RA has been well controlled till now (Fig. 3).
Discussion
So far, there have been several reports on tocilizumab-related liver toxicity. Maini et al. [3] reported AST elevation in a sawtooth pattern and ALT elevation in a dose-related manner in patients receiving tocilizumab mono-therapy. However, in their report, the cutoff for the elevation of liver enzymes was set at 100 IU/L, which was too low to be considered clinically significant. Also Smolen et al. [5] reported that 5-6% of patients receiving tocilizumab had liver enzymes elevated more than 3 times as high as the upper limit of the normal range, and elevation of more than 5 times was observed in only 1%. However, to our best knowledge, there was no report on significant tocilizumab-related liver toxicity in Koreans.
Liver biopsy in patients with tocilizumab-related hepatitis show controversial findings: Alfreijat et al. [7] reported hepatocellular necrosis and focal bile stasis, which were more likely compatible with acute liver injury by direct toxicity of the drug rather than regeneration pathway blockage. Quick recovery after discontinuation of the drug favors this explanation. On the other hand, Mahamid et al. [8] reported a case of sub-acute liver toxicity after tocilizumab treatment, and liver biopsy showed no focal necrosis; however, mild inflammatory cell infiltration and much elevated caspase 3 antigen positive hepatocytes were noted, suggestive of apoptosis rather than necrosis.
Paradoxically, IL-6 plays a major role in liver regeneration [9] and the results of the latter report could be strongly associated with cytokine-related liver regeneration. Some case reports have demonstrated severe liver injury [810], although in most studies, elevations in aminotransferase were not accompanied by other signs of hepatitis or by elevation of serum bilirubin and alkaline phosphatase levels. No cases have shown clinically significant hepatic dysfunction [345]. In several studies, an increase in serum aminotransferase levels due to tocilizumab treatment declined and normalized spontaneously without recurrent increase after the resumption of treatment. Schiff et al. [11] reported that 1.6% of patients experienced a dose reduction from 8 mg/kg to 4 mg/kg, and 2.3% of patients withdrew tocilizumab. However, no clinically relevant effect was reported on direct bilirubin, albumin, and alkaline phosphatase, and no evidence of clinically significant hepatitis was seen.
There have been several reports on the effect of tocilizumab on MAS [12], and tocilizumab stimulated rapid improvement on the clinical course of MAS in this case. However, it is unclear whether tocilizumab affects the resolutions of MAS directly or indirectly by quenching the inflammation of RA, an underlying condition known to provoke MAS. In patients with MAS, the function of natural killer cells (NK cells) is reported to be diminished [13]. NK cell dysfunction is responsible for sustained antigenic stimulation, resulting in persistent antigen-driven T-cell activation and cytokine release. These alterations in immunologic homeostasis can stimulate and sustain macrophage activation, leading to the production of pro-inflammatory cytokines, such as TNF-a, IL-1, and IL-6, at high levels [14]. For this reason, tocilizumab might be a good therapeutic option in patients with RA who show inadequate response to antirheumatic drugs and those in whom MAS is suspected.


 XML Download
XML Download