

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Viral infection, drugs, or autoimmune hepatitis are the primary causes of acute liver injury (ALI). Malignant infiltration is a relatively uncommon etiology and is usually secondary to lymphoma or leukemia [12]. Hepatic metastases of solid tumors usually have a chronic presentation instead of an acute deterioration of hepatic function, and they rarely cause ALI. Therefore, severe ALI in patients receiving chemotherapy is most likely due to either drugs or acute viral hepatitis. We report the case of a patient with colon cancer who presented with ALI caused by lymphangitic liver metastasis.
Case
A 56-year-old man was diagnosed with cancer of the ascending colon along with retroperitoneal lymph node and peritoneal metastases. Following palliative right hemicolectomy, pathological examination revealed a moderately differentiated adenocarcinoma. Postoperative computed tomography (CT) revealed newly developed metastases to the liver and superior mesenteric lymph nodes. Liver function test values were as follows: serum aspartate aminotransferase (AST), 30 IU/L (normal range, 0 to 40 IU/L); serum alanine aminotransferase (ALT), 36 IU/L (normal range, 0 to 40 IU/L); serum alkaline phosphatase (ALP), 193 IU/L (normal range, 40 to 129 IU/L); and total bilirubin 0.5 mg/dL (normal range, 0.2 to 1.2 mg/dL). He was enrolled in a phase-II clinical trial of palliative triplet chemotherapy with S-1, irinotecan, and oxaliplatin. After two treatment cycles, CT showed partial responses of the hepatic and lymph node metastases.
His liver function test values abruptly changed after six cycles of chemotherapy, with AST 203 IU/L, ALT 147 IU/L, ALP 274 IU/L, and total bilirubin 1.1 mg/dL. CT of the liver showed progressive disease with enlarged retroperitoneal and perigastric lymph nodes, but without morphological abnormalities, including biliary tract dilatation. The previously noted hepatic metastases were nearly invisible. Chemotherapy-related toxic hepatitis was suspected, and all treatment was postponed for 1 week.
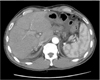
One week later, he presented with progressive jaundice with AST 168 IU/L, ALT 159 IU/L, ALP 638 IU/L, and total bilirubin 6.4 mg/dL on admission. Obstructive jaundice because of the compressive metastatic lymph nodes was strongly suspected, but CT showed only hypoattenuation along the periportal area without biliary tract dilatation (Fig. 1). Endoscopic retrograde cholangiography on hospital day 2 showed a tight stricture of the proximal common bile duct. Endoscopic sphincterotomy and biliary stenting into the common bile duct was performed. However, the total bilirubin level continued to increase even after sphincterotomy and rose to 16.7 mg/dL on hospital day 8. Abdominal ultrasonography did not show biliary duct dilatation but showed an increase in ascites. Blind liver biopsy was performed on hospital day 10 because a hepatic parenchymal pathological process, rather than biliary tract obstruction, was suspected.
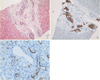
The biopsy specimen revealed tumor infiltration along the liver lymphatics (Fig. 2A). Strongly positive cytokeratin (CK)-20 immunostaining (Fig. 2B) suggested that the tumor cells had a colonic origin. The hepatic parenchyma and sinusoids were not involved; moreover, immunostaining with D2-40, anti-lymph duct endodermis antibody, showed that tumor cells were mainly confined within the lymphatic vessels and were absent from the arteries and veins (Fig. 2C).
Palliative cetuximab and radiotherapy were administered after the liver biopsy, but his performance status continued to deteriorate with a gradual onset of drowsiness, which suggested hepatic encephalopathy. On hospital day 20, total bilirubin level had increased to 46.4 mg/dL, ALP was 1,538 IU/L, prothrombin time (PT) international normalized ratio (INR) was 1.30, albumin was 3.5 g/dL, AST was 377 IU/L, and ALT was 241 IU/L. The patient died because of disease progression on hospital day 22.
Discussion
Hepatic metastases from extrahepatic malignancies usually show a hematogenous spreading pattern. Most present as multinodular lesions, but diffuse intrasinusoidal metastases have been rarely reported in lymphoma, leukemia, small cell lung cancer, breast cancer, or urothelial cancer [34]. Lymphangitic hepatic metastases are even rarer, with reports of a few cases arising from gastrointestinal cancer. Itoh et al. [5] reported lymphangitic metastases in 10 (4%) of 250 autopsied cases with liver metastases, including eight patients with gastric cancer, one with pancreatic cancer, and one with gallbladder cancer. Microscopic examination revealed retrograde spread of tumor cells from the large hilar lymphatics to the periphery along with numerous tumor emboli within the dilated lymphatics. This pattern of lymphangitic metastases can cause portal vein, hepatic artery, and bile duct obstruction [56]. In our case, blind liver biopsy showed that tumor cells were confined within lymphatic vessels in the interstitium, not sinusoidal spaces, and the hepatic parenchyma was free of tumor involvement. These findings are consistent with lymphangitic liver metastasis. To our knowledge, this is the first reported case of lymphangitic spread of colon cancer to the liver.
Differential diagnosis of acute hepatic injury without significant radiological morphological changes in liver includes hepatitis, fatty infiltration, glycogen storage disease, amyloidosis, passive congestion, and diffuse lymphangitic metastasis, as in this case. Lymphangitic liver metastasis is hard to diagnose radiologically. On CT, the slender and irregularly shaped areas of low attenuation around portal branches, i.e., the "periportal collar," can be observed; these findings were noted in this case as well (Fig. 1). This finding correlates with dilated lymphatics, and is considered a characteristic finding of lymphangitic metastasis to the liver [7]. However, these radiological characteristics are typical not only of lymphangitic metastases but also of hepatic lymphedema because of cirrhosis or congestive heart failure. On magnetic resonance imaging (MRI), lymphangitic metastasis is associated with a prominent geographic signal drop on T2-weighted imaging after the administration of superparamagnetic iron oxide [8]. However, deterioration of our patient's condition prevented further workup with MRI.
We conclude that diffuse lymphangitic liver metastasis might be considered with other differential diagnoses in patients with a history of colorectal cancer presenting with progressive jaundice without biliary tract dilatation or other clinically consistent morphological changes. In such patients, radiological findings are rarely specific for the diagnosis of lymphangitic metastasis, and blind liver biopsy should be considered in highly suspicious cases.
 XML Download
XML Download