

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The human epidermal growth factor receptor 2 (HER2) is the ErbB family of receptor tyrosine kinase. It participates in cell growth processes [1]. For activation of cell signaling, HER1, HER3, and HER4 need to bind with ligand but HER2 can be activated without ligand binding [2]. Without treatment, HER2-positive breast cancers are associated with an inferior prognosis [3].
Recently, metastatic HER2-positive breast cancer is preferably treated with the standard pertuzumab plus trastuzumab plus taxane regimen. A randomized, double-blind, phase III study compared the efficacy and safety of pertuzumab in combination with trastuzumab and docetaxel versus trastuzumab and docetaxel as first-line treatment for metastatic HER2-positive breast cancer. The addition of pertuzumab provided a statistically significant improvement in the progression-free survival (PFS) compared to that obtained with trastuzumab plus docetaxel alone. The median independently assessed PFS was 12.4 months in the control group and 18.5 months in the pertuzumab group [4].
Trastuzumab-exposed metastatic HER2-positive breast cancer is preferably treated with ado-trastuzumab emtansine (T-DM1). T-DM1 is an antibody-drug conjugate. A recent randomized international, multicenter, open-label, phase III study evaluated the safety and efficacy of T-DM1 compared with lapatinib plus capecitabine regimen for patients with HER2-positive patients with locally advanced or metastatic breast cancer [5]. T-DM1 demonstrated a statistically significant improvement in both primary endpoints of PFS and overall survival (OS). The PFS was 9.6 months with T-DM1 and 6.4 months with lapatinib plus capecitabine regimen. On the first interim analysis, T-DM1 also demonstrated significantly improved OS [5].
On the other hand, lapatinib plus capecitabine regimen has been approved since 2007 for metastatic HER2-positive breast cancer patients who had pretreated with anthracycline, taxane, and trastuzumab[6]. However, a phase III study, compared lapatinib plus capecitabine with capecitabine alone in women with advanced or metastatic breast cancer refractory to trastuzumab, revealed only one complete response case of 324 cases [6]. Recently, we experienced a patient who had a metastatic HER2-positive breast cancer with heavily pretreated trastuzumab-resistant pulmonary and pancreatic metastases and achieved a long-term complete response with lapatinib plus capecitabine combination.
Case
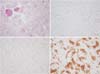
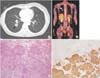
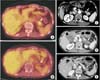
A 37-year-old woman was diagnosed with invasive ductal carcinoma of the right breast (Fig. 1). She underwent a total mastectomy and axillary lymph node dissection in May 2003. The tumor measuring 1.1 cm had no nodal or distant metastasis (pT1N0M0, stage I according to the 7th American Joint Committee on Cancer). Also it was an estrogen receptor-negative, progesterone receptor-negative and HER2-positive tumor with low Ki-67 index (5%), as determined by immunohistochemistry assay. She received six cycles of adjuvant chemotherapy (cyclophosphamide, methotrexate, and 5-fluorouracil). In January 2007, a solitary pulmonary nodule, which was 1.8 cm in diameter, was detected on chest computed tomography (CT) (Fig. 2A); it was confirmed to be a metastasis from the breast via percutaneous needle aspiration. There was no other distant metastasis except for a single mass in the right lung on 18F-fluorodeoxyglucose positron emission tomography-CT (18F-FDG PET-CT) (Fig. 2B). Lobectomy of the right lower lobe was performed via open thoracotomy (Fig. 2C, D). Six cycles of paclitaxel plus trastuzumab were then administered, followed by 35 cycles of trastuzumab until progression. In March 2009, the pancreatic lesion was detected on 18F-FDG PET-CT with standardized uptake value of 7.7 (Fig. 3A). The mass was observed as a low attenuating lesion (1.5 cm) in the pancreatic head on a CT scan of the abdomen and pelvis (Fig. 3B). A pylorus-preserving pancreaticoduodenectomy was performed, and metastatic infiltrating ductal carcinoma was confirmed (Fig. 3C, D). She received two cycles of combination chemotherapy with doxorubicin and cyclophosphamide. And newly appeared small lymph nodes at the mesentery were detected, considered disease progression. Therefore, eight cycles of gemcitabine and navelbine were administered from June to November 2009. However, in May 2010, a metastatic lesion of the pancreatic tail was newly detected on 18F-FDG PET-CT (Fig. 4A), and the nodules in the mesenteric lymph nodes became unremarkable. This pancreatic tail lesion was 1.5 cm in diameter on the CT scan (Fig. 4C). She received image-guided radiation therapy (IGRT) of 45 Gy in three fractions but the mass increased to 4 cm, as observed on a CT scan obtained the next month (Fig. 4D). Lapatinib plus capecitabine regimen was initiated in July 2010, and these treatments were continued over 4 years. The pancreatic tail lesion disappeared on an 18F-FDG PET-CT scan obtained in January 2011 (Fig. 4B) and on an abdominal-pelvic CT scan obtained in May 2011 (Fig. 4E). The pancreatic tail mass has been in complete response for 48 months since May 2011. A 25% dose reduction of lapatinib from the original dose was done in only one cycle due to grade 2 hyperbilirubinemia. The dose of capecitabine was reduced by 25% from the 3rd to 26th cycles due to grade 2 diarrhea and has been administered at 60% of the original dose from the 27th cycle until now.
Discussion
Breast cancer is the most common cancer in women in the developed world. However, few patients have stage IV disease at diagnosis, and a small proportion of patients with early breast cancer will experience distant metastatic relapse. In metastatic breast cancer at initial diagnosis or at recurrence, systemic chemotherapy is generally used. However, some metastatic breast cancer patients with oligometastatses (OM) should be managed by multimodal treatments with dedicated specialists [7]. The OM state implies that a few metastases (usually ≤5) exist before tumor cells acquire widespread metastatic potential [8]. Improvements in surgical and radiation techniques, the development of new tools to deliver local chemotherapy, and new procedures enable the careful consideration of single and combined modalities.
A recent prospective German series of patients with lung metastases (n=81) showed that R0 resection (achieved in 81.5% of patients) was associated with a significantly longer median OS than R1/R2 resections (103.4 vs. 23.6 vs. 20.2 months, respectively; P<0.001). Multivariate analysis results showed that R0 resection, number (=1), size (<3 cm), and hormone receptor positivity of metastases are independent good prognostic factors for long-term survival [9].
Pancreatic metastases from breast cancer are rare, with a reported rate of 13% in an autopsy series [10]. So in the case of pancreatic metastases from breast cancer, it is difficult to establish the disease course without surgical resection and assess the real survival benefit after metastasectomy. However, for some patients with limited pancreatic disease, surgical resection could be a palliative treatment associated with chemotherapy, hormonal therapy, and radiation therapy (RT) in the multimodal treatment of metastatic breast cancer.
Retrospective data revealed that administration of RT to the metastatic sites may be associated with better survival [7]. In the last decade, different forms of highly conformal RT such as stereotactic body RT, IGRT, and radiosurgery, have been highlighted as potentially curative therapeutic strategies for localized lesions [7].
Therefore, our patient who had OM underwent two metastasectomies, IGRT and systemic chemotherapies were administered. And finally, the patient achieved a complete response with lapatinib plus capecitabine regimen and she is being in long-term cancer-free with continuation of this combination.
Lapatinib plus capecitabine regimen has several advantages. All of two drugs in this regimen are orally active and less toxic agents than other chemotherapeutic agents for HER2-postivie breast cancer [6]. In addition, we can anticipate central nervous system response from this combination. Trastuzumab does not cross the blood-brain barrier. Therefore tumors could disseminate and grow in the brain during trastuzumab therapy. However, lapatinib plus capecitabine is effective for previously untreated brain metastatic patients with metastatic HER2-positive breast cancer [11]. Central nervous system response was noted in two-thirds of patients, and among them about a fifth having a size reduction of >80% [11]. In comparison, whole-brain RT alone response rate was 27% in brain metastatic breast cancer patients at 3 months [12].
If lapatinib plus capecitabine regimen fails in this patient, we can choose other HER2-targeted therapies or new drugs. Pertuzumab is a humanized monoclonal antibody that prevents receptor dimerization between HER2 receptors and between HER2 and other family members such as HER1, HER3, and HER4 [4]. T-DM1 consists of trastuzumab bound by a stable thioether linkage to a derivative of maytansine, a microtubule-binding chemotherapeutic agent. In response to antibody binding, the emtansine molecule is selectively released into a tumor cell, where it acts on the microtubules within the nucleus [5]. Tanespimycin is an inhibitor of heat shock protein 90 (HSP90), which is responsible for the conformational stabilization of HER2 [13]. HSP90 inhibition leads to proteasomal degradation of the HER2 protein [13]. Neratinib is an oral irreversible small molecule tyrosine kinase inhibitor of HER1, HER2, and HER4 [13].
In conclusion, our case suggests that there is a small subpopulation among HER2-positive metastatic breast cancer patients who can achieve a long-term cancer-free interval through aggressive multimodal treatments including surgery, radiation and long-term continuation of effective anti-HER2 therapies such as lapatinib plus capecitabine combination. The development of new drugs containing targeting agents is a promising medical breakthrough, that may contribute to increase survival rate of patients with breast cancer.

 XML Download
XML Download