

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Simultaneous thrombotic occlusion of two or three coronary arteries in acute myocardial infarction (AMI) is very rare and has poor prognosis [12]. Therefore it is very important to recognize this condition and provide both prompt and appropriate management for the patients. We report a case of AMI which was angiographically proven to be three-vessel coronary artery total occlusions.
Case
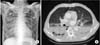
A 70-year-old Korean male arrived our emergency room (ER) for dyspnea and chest pain after losing consciousness. He had hypertension and had smoked been smoking 1 pack of cigarettes per day for 50 years. His electrocardiogram (ECG) showed non-specific ST-T change, except ST elevation in aVR (Fig. 1A), and cardiac biomarkers were within the normal range. A chest X-ray and computerized tomography (CT) revealed pneumonic consolidation on both lower lobes (Fig. 2). After endotracheal intubation, he was admitted to the Intensive Care Unit (ICU) due to pneumonia and respiratory failure.
After six hours from the initial ECG, sudden ventricular tachycardia occurred and then became an asystolic state (Fig. 1B). We performed cardiopulmonary resuscitation (CPR) with cardioversion for about 30 minutes, and his spontaneous rhythm was recovered. With hemodynamic support including inotropics, his blood pressure was 80/50 mmHg with a pulse rate of 95/min. The ECG showed ST elevation on V1-3, aVR (Fig. 1C), which suggested anteroseptal wall MI. In addition, cardiac biomarkers were elevated at the level of troponin I 5.92 (normal, 0 to 0.05 ng/mL) and CK-MB isoenzyme 52.89 (normal, 0 to 3.6 ng/mL).
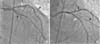
An urgent coronary angiogram (CAG) revealed three-vessel coronary disease; total occlusions of the proximal left anterior descending artery (LAD), the proximal left circumflex artery (LCX) and the proximal right coronary artery (RCA) (Fig. 3). Fortunately, the flow to the diagonal artery (D1) from LAD was preserved with thrombosis in myocardial infarction (TIMI) flow II. We inserted intra-aortic balloon pump (IABP) first and undertook percutaneous coronary intervention (PCI) on the proximal LAD, which was the culprit vessel for this ST-elevation myocardial infarction (STEMI). The LAD lesion was passed easily and smoothly with a 0.014 floppy guidewire (Balanced Middle Weight, Abbott Vascular, Santa Clara, CA, USA). An everolimus-eluting stent (Xience prime, Abbott Vascular). 3.0×23 mm was deployed after ballooning, resulting in TIMI flow III, but did not show any collateral flow from LAD to LCX territory (Fig. 4). We moved to the second intervention of the proximal LCX. The proximal LCX lesion also was passed easily with a 0.014 floppy guidewire. Another Xience prime stent 3.0×33 mm was deployed and well positioned after ballooning. After the successful intervention on the proximal LCX, TIMI grade III flow was obtained without complication (Fig. 4). Multiple fine collaterals were suspected from left coronary arteries to RCA territory, but we had no time to check collateral flow due to the patient's hemodynamic status.
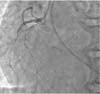
We attempted to perform the third intervention on the proximal RCA, but the lesion was so hard that we failed to pass through the lesion with a 0.014 floppy guidewire (Fig. 5). Furthermore, he was in a critically unstable condition as he recovered from sudden cardiac arrest, so we finished the intervention. During the angiogram and intervention, his blood pressure was maintained at about 90/60 mmHg with hemodynamic support including inotropics and IABP. It took about 50 minutes to finish the entire procedure in the angioroom.
On the next day, echocardiography revealed global hypokinesia with a left ventricular ejection fraction of 25%. The serial cardiac enzyme reached the peak level on the 3rd hospital day, and normalized on the 7th hospital day. However, during the prolonged ICU stay, he suffered from recurrent pneumonia with multiple organ failure and recurrent VT episodes. In spite of the treatment with broad-spectrum antibiotics and anti-arrhythmics such as lidocaine and amiodarone, he eventually died on the 58th hospital day.
Discussion
AMI with simultaneous occlusion of two or three coronary arteries is very rare [12]. Patients with simultaneous multivessel coronary thrombosis have more severe clinical outcomes, including death [12]. The concomitant coronary chronic total occlusion (CTO) in the non-culprit artery is an independent predictor of mortality [3], and failed PCI of CTO is a marker of a worse long-term outcome [4].
In our case, when the patient arrived at the ER, he complained of chest pain. However, we could not find any evidence of AMI before sudden cardiac arrest occurred. After successful resuscitation, his ECG showed AMI involving LAD. However, the CAG revealed total occlusions of LAD, LCX, and RCA, which were more severe than we expected. Although the initial ECG showed ST elevation in aVR, which might suggest global subendocardial ischemia of the left ventricle [5], we focused on the possibility of myocardial ischemia due to decreased myocardial perfusion, which resulted from a septic state rather than multi-vessel coronary disease. If we considered all possible causes of ECG change in a balanced way, the patient might have a better outcome in hospital stay. Although bypass surgery is preferred in multi-vessel coronary thrombosis, including a proximal LAD lesion, we performed emergency PCI because cardiac surgery is impossible in our hospital. Immediate angioplasty on the LAD and LCX were done successfully, and IABP was inserted within 3 hours from the time of sudden cardiac arrest, although the angioplasty of RCA failed. However, he recovered better than we expected until complicated pneumonia recurred on the 30th hospital day. We believe that early reperfusion therapy and consequent TIMI III flow after PCI would contribute to his clinical course. We thought that recurrent VT episodes were a factor in multiple organ failure.
The pathophysiologic conditions causing multiple coronary thromboses are uncertain. Possible mechanisms of multi-vessel coronary thrombosis have been suggested, including multiple plaque rupture with diffuse inflammatory process "pan-arteritis" [6], decreased blood flow to other coronary arteries after single territory STEMI [6] and systemic inflammation [7], the state of hypercoagulability [8]. Smoking is also related to an increased risk of coronary artery thrombosis by accelerating platelet aggregation and adhesion and by impairing endothelium dependent vasodilation [9]. In our case, the patient had the risk factor of coronary artery disease, including hypertension and smoking, and he was in systemic inflammation with pneumonia which might be involved in the development of acute simultaneous occlusions of LAD and LCX by causing a hypercoagulable state as well as CTO of RCA.
These simultaneous thromboses of the left coronary arteries were supported by angiographic findings that both lesions were passed easily by soft guidewire, and there were no collateral flows from other vessels to LAD and LCX territories. However, RCA lesion would be considered as CTO, as it was too hard for the guidewire to pass through, and multiple fine collaterals from the left coronary arteries to RCA territory were suspected after intervention.
In conclusion multiple coronary artery occlusion in AMI area is very rare, but a life-threatening condition. Moreover, it is not easy to differentiate multi-vessel coronary thrombosis in the clinical settings. If we had recognize such condition and provide timely and appropriate management, we might have an important influence on the prognosis of patients with multi-vessel coronary artery thrombosis.


 XML Download
XML Download