

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Adrenocortical insufficiency is the clinical manifestation of deficient production or action of glucocorticoids. It is a life-threatening disorder that can result from primary adrenal failure or secondary adrenal failure due to impairment of the hypothalamic-pituitary axis. Primary adrenocortical insufficiency can be caused by autoimmune adrenalitis, infection (especially, tuberculosis), metastatic cancer, lymphoma, adrenal hemorrhage, infarction or drugs. Among these, adrenal hemorrhage may be caused by anticoagulant drug or heparin therapy, thromboembolic disease, hypercoagulable states such as antiphospholipid syndrome, physical trauma, postoperative state, sepsis and severe stress from any cause. However, even fewer reports exist of adrenocortical insufficiency due to spontaneous bilateral adrenal hemorrhage. We report a rare case of acute adrenocortical insufficiency due to spontaneous bilateral adrenal hemorrhage presenting as acute abdominal pain.
Figures and Tables

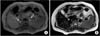
 | Fig. 2Contrast-enhance abdominal computed tomography (CT). CT scan shows low-attenuation masses in both adrenal glands (arrow).
|

References
1. Addison T. On the constitutional and local effects of disease of the supra-renal capsules. London: Samuel Highley;1855.
2. Charmandari E, Nicolaides NC, Chrousos GP. Adrenal insufficiency. Lancet. 2014; 383:2152–2167.
3. Arlt W, Allolio B. Adrenal insufficiency. Lancet. 2003; 361:1881–1893.
4. Rosenberger LH, Smith PW, Sawyer RG, Hanks JB, Adams RB, Hedrick TL. Bilateral adrenal hemorrhage: the unrecognized cause of hemodynamic collapse associated with heparin-induced thrombocytopenia. Crit Care Med. 2011; 39:833–838.
5. Espinosa G, Santos E, Cervera R, Piette JC, de la Red G, Gil V, Font J, et al. Adrenal involvement in the antiphospholipid syndrome: clinical and immunologic characteristics of 86 patients. Medicine. 2003; 82:106–118.
6. Rao RH, Vagnucci AH, Amico JA. Bilateral massive adrenal hemorrhage: early recognition and treatment. Ann Intern Med. 1989; 110:227–235.
7. Feuerstein B, Streeten DH. Recovery of adrenal function after failure resulting from traumatic bilateral adrenal hemorrhages. Ann Intern Med. 1991; 115:785–786.
8. Stewart PM, Krone NP. The adrenal cortex. In : Melmed S, Polonsky KS, Larsen PR, Kronenberg HM, editors. Williams textbook of endocrinology. 12th ed. Philadelphia, PA: Saunders Elsevier;2011. p. 479–544.
9. Xarli VP, Steele AA, Davis PJ, Buescher ES, Rios CN, Garcia-Bunuel R. Adrenal hemorrhage in the adult. Medicine. 1978; 57:211–221.
10. Kovacs KA, Lam YM, Pater JL. Bilateral massive adrenal hemorrhage: assessment of putative risk factors by the case-control method. Medicine. 2001; 80:45–53.
11. Swyer GI. Addison's disease. Br Med J. 1979; 2:25–26.
 XML Download
XML Download