

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Laparoscopic sleeve gastrectomy can reduce morbidity and mortality in patients with morbid obesity, but it can cause complications such as a gastrointestinal leak. A 30-year-old morbidly obese female who had type 2 diabetes mellitus and hypertension with estimated body mass index of 40.2 kg/m2 was admitted. Laparoscopic sleeve gastrectomy was performed. On postoperative day 19, a leak was suspicious on physical examination and radiologic findings. Conservative management was performed, but the patient was hemodynamically unstable and imminently septic. After laparoscopic drainage procedure, esophagogastroduodenoscopy was performed and revealed the fistula opening at staple line just below gastroesophageal junction. Fibrin tissue adhesive was injected around the fistula and the esophageal covered stent was inserted to cover the leak. At 14th days after stent insertion, the barium study confirmed no more leak. In this case, we experienced that the esophageal stent insertion with fibrin tissue adhesive injection may reduce recovery time of the fistula developed after laparoscopic sleeve gastrectomy.
Figures and Tables
Fig. 1
Abdominal computed tomography findings. (A) Leak at anastomosis site are seen on postoperative day 19 (arrow). (B) Leak is not improved in spite of percutaneous drainage.
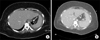
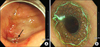
Fig. 2
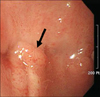
Endoscopic findings. (A) Postoperative leak is noted at upper sleeve site (arrow). (B) Esophageal covered stent was placed on postoperative day 24.
References
1. Korea Centers for disease Control and Prevention. 2011 Korea National Health and Nutrition Examination Survey [Internet]. Cheongwon: Korea Centers for disease Control and Prevention;2012. cited 2013 Aug 7. Available from: http://knhanes.cdc.go.kr/knhanes/index.do.
2. Lee JM. Body weight change of Korean. Press release of Ministry of Health and Welfare [Internet]. Seoul: Ministry of Health and Welfare;2012. cited 2013 Aug 7. Available from: http://www.mw.go.kr/front_new/al/sal0301vw.jsp?PAR_MENU_ID=04&MENU_ID=0403&page=39&CONT_SEQ=277826.
3. Oshiro T, Kasama K, Umezawa A, Kanehira E, Kurokawa Y. Successful management of refractory staple line leakage at the esophagogastric junction after a sleeve gastrectomy using the HANAROSTENT. Obes Surg. 2010; 20:530–534.
4. Fuks D, Verhaeghe P, Brehant O, Sabbagh C, Dumont F, Riboulot M, et al. Results of laparoscopic sleeve gastrectomy: a prospective study in 135 patients with morbid obesity. Surgery. 2009; 145:106–113.
5. Burgos A, Braghetto I, Csendes A, Maluenda F, Korn O, Yarmuch J, et al. Gastric leak after laparoscopic-sleeve gastrectomy for obesity. Obes Surg. 2009; 19:1672–1677.
6. Casella G, Soricelli E, Rizello M, Trentino P, Fiocca F, Fantini F, et al. Nonsurgical treatment of staple line leaks after laparoscopic sleeve gastrectomy. Obes Surg. 2009; 19:821–826.
 XML Download
XML Download