

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Adolescent addictive behaviors use continues to be a grave societal concern[1]. Adolescent who have addictive behaviors are at risk for many adverse consequences, including delinquency, poor academic achievement, employment problems and criminal and violent behaviors[2]. And most addictive behaviors such as gambling and alcohol abuse are a gateway other addictive behaviors or perhaps an enhancer of existing addictive behavior[3]. Also the problem of adolescent behavior can be connected to an adult problem[4], so the prevention interventions against youth addictive behaviors are needed.
The important one of the predictors for prevent adolescent addictive behaviors was the reported one of the predictors for social support such as positive communication with parents, peer and social group[5,6]. And the proper human resources for facilitator for adolescent addiction prevention was experts roles in school and community[7]. Park and Jung[7] found that we concludes that plan for the integration of the family, school, and community systems are a promotion of the roles, a feedback to strengthen the roles, sharing of awareness of problems, and constant effort to secure policy support. Thus, community's the most important roles for prevent adolescent addictive behavior were professional therapy and support by experts. Therefore, we must be watched with deep concern to expert competency for prevent adolescent addictive behavior. However, no studies of which we are aware have examined expectancies as expert competency for prevent adolescent addictive behavior.
Competency modeling is considered what to know expert competency for preventing adolescent addictive behavior. Competency modeling is an important innovation that it is way to get organization to pay attention to job-related information and employee skill in management of employees[8]. And competency modeling are usually directly linked to work objectives and strategies and may consider future work requirement either directly or indirectly[9]. Competency models can play many in human resource system and nursing education[6,8,10]. For example, executive development and coaching programs often have a competency model foundation[9,11]. And the best practice in competency modeling are analyzing competency information, organizing competency information, and using competency information[9,11]. There are other methods that are unique to competency modeling by behavioral event interview[11]. However, a competency modeling was using additional unique methods by the expert's delphi method[9,11]. The expert's delphi method of competency modeling was using to definite experts's competency - knowledge, skill, abilities, motivation, beliefs, values and interests - and oriented work role requirements and education[12,13]. So we can be used to identify expert competency for preventing adolescent addictive behavior and to provide an education plan to reinforcement the experts' competency.
Educational needs analysis of competency is a way what to reinforcement the experts' competency. Many research in education[13,14,15] and counseling[16] was consisted to experts' training programs according to analyse educational need of competency. And the studies about the global health education[17] and the psychiatric mental health nurse for mental illness care was performed some researchers. However, no studies of which we are aware have consisted to education program for experts such as psychiatric mental health nurses competency for preventing adolescent addictive behavior.
In this study, we want to develop the expert competency model for preventing adolescent addictive behavior by the expert's delphi method and to analyse validity in he expert competency model. And this study tries to analyse educational needs of psychiatric mental health nurses about the expert competency for preventing adolescent addictive behavior, and to provide a base for psychiatric mental health nurses to reinforcement the competency for adolescents' mental health. The purpose of this study was to develop the expert competency model for prevent adolescent's addictive behavior and to analyse educational needs of psychiatric mental health nurses that will identify a education problem to psychiatric mental health nurses in Korea.
METHODS
1. Methodology
1) Development of expert competency model for preventing adolescent addictive behavior
(1) Delphi for panelists
The study was exploratory and descriptive. Its goals were to collect expert competency for preventing adolescent addictive behavior. First, A Classic Delphi technique with three iterations [10] via web delivery was utilized. Panelists were those with acknowledged expertise in adolescents' mental health management or counselor. Panelists consisted of 3 psychiatrists, 3 professors of nursing, 5 psychiatric mental health nurses, 5 clinical psychologists, 5 counselor teachers, 2 social workers.
Round 1
The first started with an open-ended questionnaire to get opinions about the competency of expert competency for preventing adolescent addictive behavior. From the data, themes were extracted for developing core competences for round 2 and 3. Open-ended questionnaire is "What is the competency of expert competency for preventing adolescent addictive behavior? And please definition to it." Panelists were asked to give as clear description of each idea as possibles by e-mail. Data analysis was undertaken by two members of the research team to identify key concepts and themes. The first survey was developed 74 competencies in 5 categories- knowledge, skill, motivation, trait, and self-concept[10].
Round 2
The second round was a structured questionnaire with items in categories and sub-categories along the lines just explained. Panel members rated the items in Round 1, using a five-point Likert-type scale from 1 point "not very important" to 5 point "very important". The second survey was developed 120 items in 6 competenciescapability of adolescents comprehension, positive selfworth, capability of inner motivation, communication skills with adolescent, problem solving skills, and addiction management skills. The 120 items was developed 6 competencies definition and concepts from 74 competencies' definition by experts' statements in round 1.
Round 3
The third round was surveyed content validity about the 120 items from the second round by panel members. Panel members rated the items in round 2, using a four-point Likert-type scale from 1 point "not very appropriate" to 4 point "very appropriate" in order to determine content validity index. 79 items was selected according to the above .83 by index of content validation[18].
(2) Validity test of competency model
This study was selected to develop scale-experts' competency scale for preventing adolescent addictive behavior - for validity test. The data collection was conducted during March, 2013 for performing this procedures. Sample sizes needed to be considered at least 2 to 10 times the number of questions[19], therefore, 445 experts on adolescence. Sampling method was convenience sampling. The setting for this study was 4 hospitals, 2 counselling centers, 4 middle and high schools and 3 mental health centers in 4 cities in South Korea. Experts consisted of psychiatrists, nurses, psychiatric mental health nurses, clinical psychologists, counselor teachers, social workers. Informed consent was obtained prior to participation from experts on adolescence. The questionnaires took 30 minutes to complete. Excluding the incomplete questionnaires, data from 441 experts on adolescence were collected and used for analysis.
2) Educational needs of psychiatric mental health nurses about expert competencies
The second study had two scales per item of experts' competencies-importance and current level of competency. Each competency was rated as to how important it was for psychiatric mental health nurses to have and the current competency level. Level of importance of the competency and current competency were rated using a five-point Likert-type scale by mental health nurses. The data collection was conducted during November, 2013. Educational Needs of psychiatric mental health nurses about experts' competencies was analyzed by formula about educational needs[15,20].

PNC: Importance of the competency
PCL: Current competency
PNC: Mean about importance of the competency
N: number of participation
2. Data analysis
The analysis were carried out using SPSS version 20.0 for Windows. Descriptive statistics were used to analyze the characteristics of the sample. Principal component analyses evaluated factor structure using varimax rotations. Cronbach's α evaluated internal consistency for the items comprising the experts' competencies. Educational needs of psychiatric mental health nurses about experts' competencies was used to analyze formula about educational needs.
RESULTS
1. Expert competency model for preventing adolescent addictive behavior
1) General characteristics of the subject
The participants in this study were 156 (35.4%) male and 285 (64.6%) female. The participants were also divided into 12 (2.7%) psychiatrists, 10 (2.3%) professors of nursing, 122 (27.7%) mental health advanced practice nurse specialists of mental health nursing, 141 (31.9%) clinical psychologists, 105 (23.8%) counselor teachers, 51 (11.6%) social workers. Duration of work experience were 203 (46.0%) above ten years and 238 (54.0%) under ten years. 245 (55.6%) experts were religious and 196 (44.4%) experts did not have any religion.
2) Exploratory factor analysis, construct validity
Construct validity was supported in the factor analysis. The Kaiser-Meyer-Olkin measure of sampling adequacy was .93. Bartlett's test of sphericity was statistically signigicant (p<.001), showing that there were some relationships among the variables. The factors were subjected to varimax rotation to maximize the dispersion of the loadings within factors so that loading a smaller number of variables more highly into each factor results in a more interpretable cluster of factors[21].
Factor analysis showed that a eight-factor was the most appropriate approach. 68 items had factor loading greater than 0.4 in total 79 items. The basic assumptions were satisfied with the value of factor loading[19]. And these eight-factors explained 62.0% of the variance. Factor 1 (addiction management skills) accounted for 16.8% of the variance (eigen value=12.77), factor 2 (communication skills with adolescents) accounted for 27.2% of the accumulative variance (eigen value=7.90), factor 3 (capability of inner motivation) accounted for 35.6% of the accumulative variance (eigen value=6.36), factor 4 (capability of adolescent comprehension) accounted for 42.4% of the accumulative variance (eigen value= 5.17), factor 5 (positive self-worth) accounted for 49.1% of the accumulative variance (eigen value=5.14), factor 6 (environment comprehension capability of adolescent) accounted for 55.4% of the accumulative variance (eigen value=4.77), factor 7 (addiction comprehension capability) accounted for 59.0% of the accumulative variance (eigen value=2.76), and factor 8 (perception of personal competence) accounted for 62.0% of the accumulative variance (eigen value=2.21). Factor 1 had 20 items, factor 2 had 10 items, factor 3 had 8 items, factor 4 had 7 items, factor 5 had 9 items, factor 6 had 7 items, factor 7 had 4 items and factor 8 had 3 items. Factor loadings are shown in Table 1 factor analysis for final items.
3) Reliability of the scale
Cronbach's α for the overall scale was .94. Reliability was also found for each of the four subscales: Factor 1 addiction management skills (Cronbach's α=.92); Factor 2 communication skills with adolescents (Cronbach's α =.91); Factor 3 capability of inner motivation (Cronbach's α=.89); Factor 4 capability of adolescent comprehension (Cronbach's α=.85); Factor 5 positive self-worth (Cronbach's α=.83); Factor 6 environment comprehension capability of adolescent (Cronbach's α=.83); Factor 7 addiction comprehension capability (Cronbach's α=.82); Factor 8 perception of personal competence (Cronbach's α=.85).
4) Expert competency model for preventing adolescent addictive behavior
Expert competency model for preventing adolescent addictive behavior were positive self-worth, capability of adolescents comprehension, environment comprehension capability of adolescent, capability of inner motivation, perception of personal competency, communication skills with adolescent, addiction comprehension capability, and addiction management skills. Positive self-worth means competency on the task which he/she attaches great importance and self evaluation including its accomplishment. Capability of adolescents comprehension means comprehension to adolescent's physical and psychological transition and understanding of major characteristics. Environment comprehension capability of adolescent means perception of the home, school and society's environment and phenomenon that adolescent is associated and awareness of the surrounding that adolescent is more likely to be exposed to addiction. Capability of inner motivation means perception and motivative factor on a sense of purpose and necessity of adolescent him/herself, family and school's effort for addiction prevention of adolescent. Perception of personal competency is that can support the adolescent and adolescent addiction issue. Communication skills with adolescent means ability to use verbal and nonverbal communication skills, sympathize and exchange the emotions and ideas in the interview with adolescent. Addiction comprehension capability means comprehension about knowledges, characteristics, symptoms and categories of addiction. Addiction management skills means perception about symptoms, side effects, expression mode and interventions of adolescent addiction (Figure 1).
2. Educational Needs of Psychiatric Mental Health Nurses about Experts' Competencies
1) General characteristics of the subject
The participants in this study were 19 (13.9%) male and 118 (86.1%) female. Duration of work experience were 49 (35.8%) above ten years and 88 (64.2%) under ten years. 77 (56.2%) nurses were religious and 60 (43.8 %) nurses did not have any religion.
2) Educational needs of psychiatric mental health nurses about expert competencies
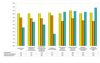
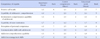
Educational needs of psychiatric mental health nurses about expert competencies for preventing adolescent addictive behavior are shown in Table 2 and Figure 2. First, importance about competency of experts was ranked communication skills with adolescents (Mean=5.0), addiction management skills (Mean=4.7), capability of inner motivation (Mean=4.7), capability of adolescent comprehension (Mean=4.6), addiction comprehension capability (Mean=4.6), environment comprehension capability of adolescent (Mean=4.6), perception of personal competency (Mean=4.6), positive self-worth (Mean=4.6). Second, current competencies about competency of experts was ranked capability of inner motivation (Mean=4.3), positive self-worth (Mean=4.0), environment comprehension capability of adolescent (Mean=3.9), communication skills with adolescents (Mean=3.9), capability of adolescent comprehension (Mean=3.9), perception of personal competency (Mean=3.5), addiction comprehension capability (Mean=3.6), addiction management skills (Mean=3.5).
Last, educational needs about competency of experts was ranked addiction management skills (Mean=5.4), communication skills with adolescents (Mean=4.9), perception of personal competency (Mean=4.8), addiction comprehension capability (Mean=4.8), capability of adolescent comprehension (Mean=3.4), environment comprehension capability of adolescent (Mean=3.0), positive self-worth (Mean=2.6), capability of inner motivation (Mean=1.7).
DISCUSSION
This study was designed to the expert competency model for prevent adolescent addictive behavior. This study examined the validity of the expert competency model for prevent adolescent's addictive behavior. Also this study was designed to analyse educational needs of psychiatric mental health nurses that will identify education problem to psychiatric mental health nurses in Korea.
First, the expert competency model for preventing adolescent's addictive behavior were positive self-worth, capability of adolescents comprehension, environment comprehension capability of adolescent, capability of inner motivation, perception of personal competency, communication skills with adolescent, addiction comprehension capability, and addiction management skills. These competences are appropriate because there are included to the competency' sub-concept as knowledge, skill, abilities, motivation, beliefs, values and interests [11]. And experts to have these competences will effectivity manage to preventing adolescents' addictive behaviors. Experts will try to reinforcement these competencies and to consider that competencies for preventing adolescent addictive behavior defined by the addiction prevention core competency model are as follows: positive self-worth, self-control skill, time management skill, reality perception skill, risk coping skill, positive communication with parents, positive communication with peer or social group[6].
Second, this study was selected to develop scale - expert competency scale for prevent adolescent addictive behavior - for validity test. Validity pertains to determine whether a scale instrument is able to make an accurate scale[22]. In this study, we used content, and construct validity.
Content validity measures the comprehensiveness and representativeness of the content of a scale[22]. Lynn[18] and Kadioglu[22] has proposed that a content validity index of at least 83% is required for an acceptable level of content validity. In our study, the overall content validity index was 83.0%, which signified that the scale has a good content validity.
Construct validity of competency model is based on the extent to which a test measures a theoretical construct or trait[23]. In this study, we excluded five items from the original scale. However, the factor load was above the set point of .40 for all selected items. The number of items for the four sub-scales which were positive self-worth, capability of adolescents comprehension, environment comprehension capability of adolescent, capability of inner motivation, perception of personal competency, communication skills with adolescent, addiction comprehension capability, and addiction management skills was 3~20. Therefore, the basic assumptions were satisfied with the number of items for each of the factors and should be included in at least three or more variables[19]. Subscales were used in this study because there was a difference in the number of questions. To determine the mean score in each subscale, further research on expert competences is necessary to obtain and analyze, and compare. But limitations of our study convergent validity isn't performed because there are no related variables.
In our study, Cronbach's α for the overall scale was .94. To measure the social scientific concept of the tool using questionnaires, Ryu[24] suggests that reliable confidence should be more than 0.70. This study resulted in a 0.90 confidence rating and so therefore, the reliability of the developed scale in this study should not be neglected. The high level of internal consistency for the entire scale indicated that computing the total score is appropriate and useful for research assisting in planning a education for expert competency program. However, because the data used in this study was cross-sectional in nature, it does not assess the sensitivity of the scale to changes over time. Future studies need to determine the test-retest reliability of the 75-item scale, whether or not the scores change over time and where it is sensitive to change date in this scale, due especially to the result of a successful experts' education program.
Last, psychiatric mental health nurses' educational needs about competency of experts was ranked addiction management skills, communication skills with adolescents, perception of personal competency, addiction comprehension capability, capability of adolescent comprehension, environment comprehension capability of adolescent, positive self-worth, capability of inner motivation. In a study about educational needs of group work supervision according to careers of grout workers, the competences of high educational needs were group dynamics and the competences of low educational needs was interaction and communication[16]. So psychiatric mental health nurses were perceived that they haven't enough management and communication skills for their clients manage. According to the psychiatric mental health nurses' educational needs about competency of experts it is considered to develop competency-based education program for preventing adolescent addictive behavior.
The findings should be viewed in light of the limitation of the study. The results can be only generalized to 2 cities in Korea. In other words, it may not be fully generalized to the Korean adolescent' mental health experts population. And another limitation is that the selected competency modeling was experts' delphi method what do not considered to the classic method with behavior event interviews. And in this study, it was analyzed mental health nurse's educational needs about experts' competency that it was not considered to the psychiatric mental health nurses' clinical levels. Despite the limitations, the present findings suggest the scale is an appropriate one for develop experts' competency model for prevent adolescent addictive behavior. This developed expert competency model and scale can improve the understanding level of the experts' current competences. Also, the competency model and scale can be used to evaluate prevention as well as experts' education programs for prevent adolescent addictive behavior in Korea.
This developed expert competency model and scale have a great validity and reliability which can evaluate characteristics of experts. Using the competency model and scale developed in this study suggests that we need to develop education program to reinforcement competences for manage to adolescents. In this study, a useful tool was developed to assess experts' competences among school, community center and medical center in Korea. The study suggests to develop effective education program based on expert competency model and educational needs for psychiatric mental health nurses.
CONCLUSION
The purpose of this study was to develop a the expert competency model for prevent adolescent addictive behavior and to analyse educational needs of psychiatric mental health nurses that will identify education problem to psychiatric mental health nurses in Korea.
In this study, the competency model and scale for experts have a significant validity and reliability, suggesting that there are a useful tool to assess competences level among experts for adolescents' mental health in Korea. More importantly, it provides the first step toward developing a education program or guideline for experts include psychiatric mental health nurses.


 XML Download
XML Download