

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Mouthrinsing as an oral hygiene measure has been practiced for thousands of years, with the first reference to it being documented in Chinese medicine in the year 2700 B.C1). Yet, it is only relatively recently that scientific and clinical evidence supporting the use of therapeutic antimicrobial mouthrinses have become available. With the recognition of the role for plaque accumulation and pathogenic oral flora in the etiology of gingivitis, the importance of plaque control and the use of effective antimicrobial agents were emphasized in preventing or reducing such inflammatory oral diseases as gingivitis2). Gingivitis is an inflammatory condition of the supporting tissues surrounding the teeth that is induced by pathogenic microorganisms and their metabolites in the dental plaque. Importantly, persistent gingivitis is a known risk factor for periodontal attachment loss and ultimately, tooth loss which can lead to diminished masticatory function and esthetics3). While the maintenance of good oral hygiene is known to be effective in controlling the plaque bacteria and gingivitis, reports indicate that the vast majority of people are unable to accomplish an adequate level of plaque control to prevent gingivitis using mechanical methods alone4). This provides a clear rationale for incorporating effective antimicrobial ad-juncts into daily oral hygiene routine, such as antimicrobial mouthrinses.
Mouthrinse formulations containing various therapeutic agents have been introduced and tested to control this inflam-matory disease of the gingiva. Antibacterial compounds such as chlorhexidine, cetylpyridinium chloride and triclosan have demonstrated some clinical efficacy but most of these chemical compounds haven been found to induce side-effects. For instance, chlorhexidine stains the teeth5) and triclosan was found to react with free chlorine in drinking water to form toxic byproducts6). As an alternative to chemical compounds, several medicinal herbs were tested for antiplaque and antigingivitis effects and some demonstrated significant clinical efficacy. Centella asiatica, also known as gotu kola, is known as a longevity herb and used as an herbal medicine in many Asian countries such as India, Nepal, China and Korea. The titrated extract of this medicinal herb is known to have anti-inflammatory, sedative and healing effects on skin wounds and is used in wound care, anti-allergy and dermatosis treatment such as leprosy and psoriasis7). It is also known to be useful for treating vascular diseases such as varicose veins and chronic venous insufficiency8). The anti-inflammatory property of this herb, in particular, is also shown to be effective in reducing plaque and gingivitis9). Magnolia bark extract is another medicinal herb used in traditional Chinese medicine for treating fever, headache, pain relief and stress reduction10). Isolated from the stem bark of Magnolia officinalis, the CO2-extracted magnolia bark extract consists of magnolol and honokiol. Experimental studies have demonstrated the antimicrobial activity of magnolol and honokiol against Helicobacter pylori, associated with gastritis and peptic ulcers11) and Propionibacterium acne, associated with skin inflammation12). Magnolia bark extract was also shown to have an antimicrobial effect on the critical pathogens of periodontal disease such as Porphyromonas gingivalis, Actinobacillus actinomycetemcomitans and Prevotella intermedia13). Bamboo salt is produced by roasting sea salt in bamboo and is widely used in Korean traditional medicine as an anti-inflammatory therapeutics14). Previous studies showed that bamboo salt is effective in relieving gingivitis151617). In addition, oil pulling is another fork remedy practiced in few countries including India for maintaining good oral health18). Yet, scientific evidence is lacking to prove its clinical efficacy on reducing dental plaque or gingivitis.
The use of antimicrobial mouthrinses as an adjunct to mechanical plaque control methods may provide an effective means of removing or controlling bacterial plaque to prevent and control gingivitis and periodontitis. However, there has not yet been a report of a comparative study on the anti-plaque and anti-gingivitis effects of oil-water two-phased and aqueous single-phased herbal mouthrinses. Thus, the aim of this study was to test new mouthrinse formulations containing bamboo salt, magnolia bark and Centella asiatica extracts in an aqueous single-phase and oil-water two-phase solutions for its clinical efficacy on reducing dental plaque and gingivitis status in Korean adults.
Materials and Methods
1. Ethical approval and clinical subjects
Ethical approval was obtained from the Institutional Review Board of Seoul National University, School of Dentistry (IRB number: S-D20140046). All participants provided a written informed consent after receiving a full explanation of the trial. This research has been conducted in full accordance with the World Medical Association Declaration of Helsinki. This study was reviewed and registered on the U.S. National Institutes of Health Clinical Trials Registry (registration number: NCT03047798; registry name: “The Effect of Mouthrinses Containing Bamboo Salt, Magnolia Bark and Centella asiatica on Reducing Plaque and Gingivitis”).
A total of 34 healthy adults from Dongjak-gu, Seoul, Korea, volunteered to participate in this study. The inclusion criteria for subjects were adults aged over 19 years with at least 20 natural permanent teeth who have mild to moderate plaque and gingivitis. For this, mild to moderate plaque was defined as having over 20% O'Leary's plaque index and gingivitis was defined as having 20 to 30% BOP rate. The exclusion criteria were as follows: individuals undergoing orthodontic treatment or having deep periodontal pockets (≥6 mm at two or more teeth) on more than two teeth, diabetics, pregnant or lactating women, taking antibiotics within the past one month or having used any mouthrinses for the past 6 months.
2. Sample size calculation
According to a precedent study on the anti-gingivitis effect of a mouthrinse, the difference in the mean pre- and post-experiment BOP index among the test group was 0.09 (0.33 at baseline and 0.24 at 3-week post-experiment) with the standard deviation of 0.2519). Under the condition of type I error at 0.05 and type II error at 0.2, the number of subjects needed for paired t-test was estimated at 12. In this study, a total of 34 volunteers were recruited to form 3 groups of 11, 11 and 12 participants (Fig. 1).
3. Study design
A randomized clinical intervention study was planned with a cross-over design. The 34 subjects were randomly allocated to one of the three experimental groups: 1) the control; 2) ASM group for aqueous single-phase mouthrinse; 3) OTM group for oil-water two-phase mouthrinse. The experimental mouthrinses all contained sodium fluoride and the ASM and OTM contained additional ingredients of bamboo salt, magnolia bark and Centella asiatica extracts (Table 1).
For the OTM, 50% essential oil was added to create an oil-water two-phase mouthrinse. Participants were instructed to use the prescribed mouthrinse to gargle their mouth after usual toothbrushing for one minute, twice daily for two weeks. Specifically, the participants were instructed to use the mouthrinse once in the morning after meal and once at night as the last thing before bed. The completion of each experiment regimen was followed by a 2-week washout period, after which the subjects of each group were permutated to the next mouthrinse trial until all three groups underwent the three mouthrinse trial regimen (Fig. 1). All 34 participants completed the experiment and hence the retention rate was 100%.
Specific oral hygiene instructions were given to study participants in order to minimize the interpersonal differences in oral hygiene routine. During the experiment, the study participants were instructed to use only the prescribed oral hygiene tools including toothbrushes, toothpastes and mouthrinses that were provided by the research group. The usage of all other oral hygiene tools including dental floss or interdental brushes were restricted during the entire experiment period. Participants were also instructed to perform toothbrushing using Bass technique. The experiment was carried out in double-blind manner for the subjects and the examiner by providing the mouthrinses in opaque white bottles, labeled “A”, “B” and “C”. Baseline and post-experiment clinical examinations were performed to measure the PI (plaque index) and BOP (bleeding on probing) for full-mouth on the first and the last days of the trial.
4. PI change
Prior to assessing the baseline PI, full-mouth professional mechanical scaling and prophylaxis were provided for the participants to remove all debris from the tooth surface. A plaque disclosing solution was used to stain dental plaque on tooth surfaces of the subjects (2Tone™ disclosing solution, Young Dental, Earth City, USA). Turesky-modification of the Quigley-Hein Plaque Index (QHPI)20) was used to assess the thickness of plaque in the gingival area of the tooth on the index teeth 11, 16, 26, 31, 36, 46.
5. BOP change
BOP is widely regarded as a relatively objective sign of gingival inflammation21). BOP was measured at the mesiobuccal, mesiolingual, distobuccal and distolingual aspects of the six index teeth namely, 11, 16, 26, 31, 36 and 46 by probing with a periodontal probe and checking for bleeding after ten seconds.
6. Statistical analysis
The average baseline and post-experiment PI and BOP are calculated as means and standard deviation for each experiment regimen. The changes in PI and BOP following each experiment were evaluated by applying the equation: Δ (%) =(Baseline mean―post-experiment mean)/Baseline mean * 100. Paired t-test was applied to compare the differences between the mean baseline and post-experiment PI and BOP for the three experiment mouthrinses. For the purpose of this analysis, a P-value<0.05 was considered a statistically significant difference.
Results
Compared to the control, both ASM and OTM showed lower post-experiment PIs (Table 2). The mean post-experiment PI for the control, ASM and OTM were 1.97, 1.94 and 1.57, respectively. However, such differences were statistically significant for neither ASM nor OTM (P>0.05).
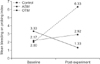
Compared to the control, significant reduction in BOP was observed in the ASM experiment group (P=0.049) (Table 3, Fig. 2). In this group, 60.1% reduction in BOP was observed following the experiment. The BOP change following the experiment with OTM was not significantly different from that of the control or ASM (P>0.05). Both the control and OTM groups showed an increased post-experiment BOP. Yet, the increment of BOP in OTM group was smaller compared to that of the control group (―34.6% compared to ―216.5% reduction ratios, respectively).
No adverse reactions were noticed clinically on soft and hard tissues of the oral cavity during the study. No subject complained of any discomfort from the use of the prescribed mouthrinses.
Discussion
Our study demonstrated that the regular use of mouthrinses containing such antimicrobial and anti-inflammatory agents as bamboo salt, magnolia bark and Centella asiatica, extracts as an adjunct to mechanical toothbrushing can alleviate gingivitis. When the formulations were tested in ASM and OTM forms, only the ASM was shown to be effective in controlling gingival inflammation.
The major strengths of our study are threefold. First, this study was designed in a randomized double-blinded manner in order to prevent potential selection or measurement bias by the examiner and recall bias by the participants. Second, this study adopted the Latin square allocation process for grouping participants into different treatment cycles to reduce the carryover problems inherent in cyclical rotation designs. Lastly, a two-week washout period was provided to also eliminate the carryover effects of the previous experiment.
Mechanical methods such as tooth brushing with toothpaste and tooth flossing are the most reliable methods to remove plaque from the surfaces of teeth. Standard recommendations for oral hygiene practices have focused on mechanical methods including tooth brushing and interdental cleaning21). Regular mechanical removal of bacterial plaque appears to be a prerequisite to prevent periodontal disease and maintain oral health22). However, a number of factors can hinder optimal tooth brushing including individuals' incompetency in toothbrushing habit, degree of periodontal tissue change due to gingivitis or periodontitis, bristle arrangement or flexibility and type of toothbrush or toothpaste23). Furthermore, a recent systematic review assessing the efficacy in dental plaque removal showed that following a single brushing exercise, the plaque reduction is only 42% on average24). Considering that such remnant plaque on tooth surfaces can cause gingivitis, the use of adjunctive cleaning agents such as mouthrinses should be integrated into oral hygiene care routine.
The results of this study showed that BOP was effectively reduced in the ASM group without concomitant decrease in the plaque index. BOP, which represents a state of gingival inflammation, indicates epithelial changes and vascular transfigurements in the gingiva surrounding the tooth, provoked by the pathogenicity of specific gingivitis-inducing bacteria including specific species of Streptococcus, Fusobacterium, Actinomyces, Veillonella, and Treponema and possibly Bacteroides, Capnocytophaga, and Eikenella25). By inhibiting the activity and growth of these pathogens in gingival crevicular spaces, the tested herbal mouthrinse could have contributed to reduced gingival inflammation. The reduction in BOP without visible reduction in the amount of supragingival plaque, implies that the down-regulating effects of the mouthrinse against the gingivitis-inducing microbial activities can take place in the presence of dental plaque. This could be possible as the gingivitis-inducing bacteria are known be active in the subgingival gingival crevicular spaces, hence not requiring meticulous plaque control on supragingival surfaces. In fact, a previous study reported that the accumulation of supragingival plaque scores demonstrated low predictability of periodontal attachment loss whereas bleeding on probing showed superior predictability during 42-month period26).
Our data supports previous studies that reported on the antibacterial and anti-inflammatory properties of bamboo salt, magnolia bark and Centella asiatica extracts. An experimental study showed that bamboo salt inhibited the secretion of such pro-inflammatory agents as tumor necrosis factor (TNF)-a, interleukin (IL)-1 beta and IL-6 to a much greater degree than the normal salt14). These inflammatory mediators are known to play vital role in inducing inflammation in gingival and periodontal tissues. An in vitro study demonstrated that magnolol and honokiol, although less potent than tetracycline, had a significant antimicrobial effect against a range of periodontopathogens13). Similar results were observed in an in vivo study in which chewing gum containing magnolia bark extract effectively reduced total oral bacteria compared to the negative controls and showed a strong antibacterial effect against known pathogens of periodontal disease including Porphyromonas gingivalis and Fusobacterium nucleatum27). In addition, an in vitro study reported that Centella asiatica extract increased the collagen synthesis in a dose-dependent manner when tested on human fibroblast cultures28). This implies that the Centella asiatica component of the mouthrinse formulation could have helped stimulate collagen synthesis within the gingival tissue and hence reducing the signs of gingival inflammation.
Intraoral oil pulling therapy has been used traditionally as a remedy for oral health maintenance and some studies showed its clinical efficacy in alleviating plaque-induced gingivitis29). In our study, the oil-water two-phase mouthrinse containing 50% essential oil did not show reduction in plaque accumulation or gingival inflammation. By creating an oil-water two-phased mouthrinse, it was expected that the active ingredients would be delivered in dissolved form. Bamboo salt compound and Centella asiatica are hydrophilic while magnolia bark extract is hydrophobic and hence both water and oil-based solvents are required as delivery medium. However, our data showed that only the mouthrinse in aqueous form was effective in reducing BOP, not the oil-water two-phased form. A possible explanation could be that the formation of micelles in oil-water mixture prevented the aqueous active ingredients from coming in contact with the tooth and gingival surfaces, hence these ingredients could not exert their anti-inflammatory effects on the gingival tissue. A meta-analysis of 6-month-or-longer clinical trials, however, showed that daily use of essential oil-containing mouthrinses statistically significantly reduced plaque and gingivitis when compared to mechanical tooth cleaning alone18). This implies that a longer trial duration could have been necessary for OTM to produce similar results.
Our study has some limitations. The two-week duration of the clinical trial could have been too short to yield sufficient result on the clinical efficacy on plaque or gingivitis control. If the trial period had been extended to three months or more, significant results could have been deduced. As aforementioned, the cross-over design of the trial inevitably involves carry-over effects which means that the effect of the previous experiment may impose influence on the following experiment. To minimize such carry-over effect, the participants underwent 14-day washout periods in-between the trial periods. Also, professional tooth cleaning was provided at the beginning of each trial prior to baseline assessment. The apparent increase in the BOP index in the control group after the experiment could be due to a couple of factors. First, the participants could have been unfamiliar with the newly-introduced Bass toothbrushing technique. The failure to comply with the correct toothbrushing method could have led to increased gingival inflammation and hence increased BOP. Second, the restricted use of other oral hygiene tools including interdental cleaning agents during the experiment could have led to increased post-experiment BOP. Reflecting back on the trial procedure, it is to our regret that there was no check on the participants' ability to correctly perform the Bass technique. However, oral hygiene instructions were re-inforced at the beginning of each trial cycle to help minimize interpersonal differences. Further study with larger number of subjects would be necessary to draw meaningful conclusions on the efficacy of these ASM and OTM.
Our study supports the evidence from previous studies that herbal extracts are effective antimicrobial and anti-inflammatory agents when used in mouthrinse formulations as an alternative to chemical compounds30). In this respect, the use of mouthrinse should be incorporated into oral hygiene routine as an adjunct to mechanical hygiene measures to facilitate the control of gingivitis.
Conclusions
ASM containing bamboo salt, magnolia bark and Centella asiatica extracts showed superior anti-gingivitis effect compared to the control and the OTM solutions. The plaque reducing effect of both the ASM and OTM were not statistically significant. Overall, for the purpose of maintaining gingival health, the authors recommend the use of this herbal ASM as an adjunct to oral hygiene care routine.




 XML Download
XML Download